Category: 2018
President’s Corner
by Cynthia Cotter, Ph.D. 
President, San Diego Psychological Association
On Saturday, October 27, 2018, the San Diego Psychological Association will present its 2018 Fall Conference entitled Encountering Substance Use in Clinical Practice: Emerging Issues and Divergent Perspectives. Mary Mulvihill, Ph.D. and I co-chaired this event; however, Dr. Mulvihill very much took the lead in the project and is the SDPA member most responsible for its production. Dr. Mulvihill put in long hours thinking through content and speakers, obtaining sponsors/exhibitors, and assisting the CE Committee in its work accrediting the courses. She also assisted in acquiring volunteers and designed the musical support for the event. Dr. Mulvihill and I thank the other members of the Fall Conference Committee, Diane Pendragon, Psy.D., Darlene Townes, Psy.D., and Rochelle Perper, Ph.D. for their very hard work. We are grateful to the members of the SDPA Addictive Disorders Committee chaired by Tom Horvath, Ph.D. and Charlie Nelson, Ph.D. for their support and assistance with the conference. The SDPA Addictive Disorders Committee is new as of 2018, and will organize moving forward the efforts of SDPA professionals with focus/interest in this highly needed specialty area.
Our association could not have chosen a more timely topic for its largest yearly continuing education event. First, there is evidence that addictions to alcohol and drugs have risen over the past twenty years, with increasingly dire consequences. Drug-related fatalities in the U.S. now exceed deaths due to breast and prostate cancer combined. A pattern of declining U.S. life expectancies has been documented and linked to what have been called “deaths of despair,” a powerful confluence of rising rates of suicide, drug overdoses, and death linked to alcohol abuse. There is speculation that something profound has happened since the 1980s to make Americans more susceptible to self-medication and its dangers.
Over 90 percent of psychologists report encountering problematic substance use in their clients. Yet psychologists often feel inadequately trained to assess, conceptualize, and treat these problems. The SDPA Fall Conference targets the clinical mental health provider who asks the following questions: How do problems related to alcohol and drugs interact with other issues/pathologies with which my client is struggling? As a generalist, can I treat addiction? When is it important to refer to specialists? Where do addiction specialists differ in conceptualizing and treating problematic substance use? Is addiction merely a habit to be behaviorally modified or are more fundamental underlying psychopathology, such as attachment injury, contributing in a meaningful way. What types of social support are most effective in treatment? Is abstinence necessary or can there be stability in moderation? Is substance use “a choice”? How do issues of pain factor in and are there meaningful treatments for pain beyond medication? The legal landscape related to marijuana use has changed. Do I respond to marijuana use in my clients with support or concern? Are problems of addiction experienced differently in people of color? How do family members factor into problems and solutions to addiction? What do I do when clients relapse? What opportunities exist for my client in use of medication assisted treatments for recovery?
This year’s Fall Conference offers continuing education credits (CMEs) for medical professionals as well as CEs for psychologists and other mental health providers, such as LMFTs, LCSWs, LEP, LPCC and RNs. CAADAC credit is also offered. We hope that general medical practitioners, internists, family physicians, psychiatrists, will join us. There has never been a time when substance use issues have been more prevalent and impactful in our clients and we must know how to best respond to these complex and compelling issues.
Articles in the current issue are a compilation of contributions from Fall Conference speakers (Dr. Writer), the SDPA Addictive Disorders Committee (Dr. Horvath, Dr. House), and significant local community substance use resources (Mr. Silverman, Dr. Barnes, Dr. Mackeogh) recruited/compiled by Dr. Mulvihill to supplement the information/education provided by the 2018 Fall Conference. We are very grateful to Dr. Mulvihill for her contributions to this issue that included designing, recruiting, following up, and editing the articles in this issue. There will be a second issue published on this topic as well as we feel that problems associated with substance use are so important and timely for mental health professionals.
![]()
It’s not too late to register for the SDPA Fall Conference of 2018!
Editorial
Welcome to the penultimate issue of 2018 San Diego Psychologist. This is the first of two issues highlighting this year’s SDPA Fall Conference entitled, “Encountering Substance Use in Clinical Practice: Emerging Issues and Divergent Perspectives.” Both issues will feature articles on topics related to the theme of the Conference, authored by experts in their field. I would like to express my deep gratitude to Dr. Mary Mulvihill, the Co-Chair of the Fall Conference. She was instrumental in shaping the content of this issue; she not only reached out to the authors of the articles for this issue, but gathered their initial drafts, did the initial edits, and arranged and conducted the interview with Dr. Silverman that is featured in this issue.
Most mental health providers have encountered patients whose problematic substance use has led to a breakdown of psychological processes and social networks. The number of people seeking substance use treatment has been dramatically rising. Substance abuse wreaks havoc on the users, their families, and their communities, costing the country approximately $740 billion as a result of crimes committed, loss of productivity, and medical expenses (National Institute on Drug Abuse). Substances of abuse range from widely prescribed medications (such as opioids and benzodiazepines) and legal (in some states, including California), recreational drugs such as alcohol and marijuana, to new illicit drugs, whose potential for harm may be yet unknown.

“Simply Addiction” (Painting by Anyes Galleani)
The first article in this issue of The San Diego Psychologist is an interview with Scott Silverman conducted by Dr. Mulvihill. Mr. Silverman is a community advocate for substance use recovery in San Diego, and has developed highly successful programs that are aimed at supporting prior substance users so that they can be contributing members of their community. The next two articles highlight two common substances with the potential for abuse, both legal in California; Dr. Writer’s myth-busting report on marijuana and its implications is in-depth and eye-opening, and Dr. Barnes addresses the alarming trend of long-term benzodiazepine prescription and use and what we as providers of therapy can do to check this dangerous practice. The last three articles focus on intervention; Dr. House makes a compelling case for psychologists (and allied mental health professionals) as the first-line providers of substance use treatment, regardless of whether they have specialized training in substance use treatment. Dr. Mackeogh discusses strategies that parents of teenagers who abuse substances can use to get them more involved in their own treatment. Finally, we are fortunate to hear from Dr. Horvath, an international leader in addiction recovery, whose SMART Recovery program that began in San Diego, is widely hailed as a successful and effective mutual support group for people trying to limit or stop substance use.
The world of substance use research and clinical practice is rife with divergent perspectives and approaches to treatment, and you may find that the articles in this issue often posit opposing views and opinions. However, the goal of each of the authors, the approaches they espouse, and the work they do is the same—to guide people back from the narrow, tragic path of substance abuse to fuller and healthier lives.
If you have comments or questions, you may directly contact the authors or email us at TheSanDiegoPsychologist@gmail.com.
Thank you for reading.
-Gauri

Dr. Savla’s private practice in Encinitas, CA is focused on seniors with aging-related challenges and/or mental illness. Before devoting her professional life to clinical service, she studied primary psychotic disorders among older adults at the University of California, San Diego and the VA San Diego Healthcare System. She has co-authored 30 peer-reviewed papers and book chapters to date. She has been the Editor of the San Diego Psychologist since 2016.
Toward New Directions in Substance Use Treatment & Recovery
An Interview with Scott Silverman, Community Advocate for Substance Use Recovery by Mary Mulvihill, Ph.D.
How did you begin your work with substance use disorders and their treatment?
For the past six years, I have been operating Confidential Recovery, an outpatient treatment center, but my community work began when I founded Second Chance, and ran it for 18 years. Second Chance is a program aimed at providing temporary residence for recently released prisoners, since it’s not possible to go to a job interview without a home address. Ex-offenders are at high risk for substance use and re-offending, and this group-oriented, social model of recovery provides a safe place to live in a substance-free environment. Clients who need substance use treatment are referred to county-funded programs. An interesting feature of the program is the “relapse house,” where a client can go if they relapse and get back on track quickly, rather than being kicked out and thus erasing all progress. Relapse is part of the disease of addiction, so the program plans for that, and does not push people out after one setback. Second Chance has 175 beds, including 30-50 on scholarship, where clients gradually earn more private accommodations in a staged housing model, using private homes the agency purchased. They are coached along the way into sobriety, job/finances training, economic self-sufficiency, and eventually, their own residence supported by full employment.
On a personal level, my own journey through recovery started 30 years ago. To recover, I had to quit working in my family business (which was killing me) and figure out another path. In my own experience, the social model is important as it helped me stay connected; I found the 12-Step Model to be very influential in this regard. I understood the process by which my own recovery worked, and from there, observed the many challenges and successes of people going through various forms of treatment, especially those who were just released from prison or homeless, and trying to stay “clean.” I kept an open mind, and began to figure out gradually how I could play a role in facilitating change for people who needed it.

What are the three biggest substance use issues in the San Diego community right now?
As substance use is becoming more prevalent, so is its impact on workplaces, homes, schools and medical settings. Particularly hard hit is the large Native American community in San Diego.
The big three substance use issues impacting San Diego currently are:
- Methamphetamine (meth) use: Local consumption of this highly destructive drug is at a 10-year high.
- Fentanyl from China, often disguised as OxyContin, along with other new synthetic drugs which are extremely dangerous, as we have no idea what is really in them. If effective at inducing a “high,” substance users tend to take more, hence putting themselves at high risk for dying from these drugs. Many of the substance-use fatalities are reported by medical examiners or morgues , rather than a medical facility, indicating sudden death. We may lose many more people to synthetic, possibly contaminated, drugs unless we get a grip on this quickly.
- Easier access to cannabis or unused prescription opiates: 264 million prescriptions for opiates were written last year, and many of them cannot be tracked down. With legalization of cannabis, we are seeing more kids overdosing, particularly with edibles. And then, there is the new issue of driving while high, which is hard to measure and control.
From your long experience in the community, what do you see as some of the main challenges facing the substance use treatment industry overall?
First, we need improved access to treatment, and incentivize going to treatment so that more substance dependent clients seek it. Part of that involves reducing the stigma associated with being an “addict” and needing “addiction treatment.”
Second, we need to hold treatment providers and insurers more accountable for the fact that substance use treatment has fairly poor results. Usually the client is blamed for treatment failure; clients are deemed “not ready” or “resistant,” “not serious,” “un-helpable” and so forth. This is a $40 billion industry, yet remains one of the few that persists in blaming the client for maladaptive behavior. I think this speaks to the stigma of substance use dependence: “It is the client’s fault.” This is so backward!
Third, there is currently no coordinated continuum of care, which is what most clients need to recover. Services are fragmented, and so poorly connected between the different levels of treatment that clients fall through the cracks. Critical information is lost from one phase to the next. The number of physicians well trained in Addiction Medicine is small, and general practice physicians have a completely different perspective to addiction and its treatment. Psychologists have a behavioral and psychological approach to treatment, which is not well understood by physicians. Professionals who are trying to work together to help the clients do not understand each other’s perspective, training, or value to the client trying to recovery. This is a mess!
Affluent clients seeking substance use recovery tend to seek out “destination” substance use recovery facilities. After completing those programs, they return to their old environment, cues, friends, and predictably, relapse. This treatment model does not work very well, yet is commonly employed, even widely accepted.
Of note, many professionals in the substance use field are themselves in recovery. Since there are no well accepted “best practices” or definitive standards for good substance use treatment, recovered professionals tend to treat their clients with the same approach they themselves used to “get clean.” This may or may not work, since every client in recovery is a bit different. Some professionals have never looked beyond the model they benefited from; their tool box may contain one or two tools, which limits its effectiveness.
Fourth, coverage and incentives by insurers or social welfare to access treatment need to be improved. Insurance coverage has declined dramatically in the last 3-5 years: In the past, a typical detox over 7-10 days within a 28-day inpatient program, followed by 4-6 weeks of outpatient therapy was the norm, whereas, today coverage is only provided for a typical 3-day detox, 14-day inpatient program, and just 2 weeks of outpatient therapy. The fog of withdrawal may not even clear by the time the client’s insurance times out. We do not know how the consensus of a 30-day treatment period was established, but we do know that this schedule does not address the intensity or the chronicity of the client’s medical problem; 95% of substance use clients in such programs will relapse. We would never treat diabetes this way.
What is your opinion of the new medically assisted therapy (MAT) as a new option for improving treatment outcome in substance use treatment? What are the barriers to implementing this approach more widely?
I think MAT is a much needed step forward, particularly, the use of long acting opioids to treat opiate addiction. Clients in withdrawal cannot cognitively or emotionally engage the way they need to in treatment to fully benefit or attain recovery. Cravings are too distracting.
There are a number of barriers. Most insurance plans only cover a few days of detox, and a recovery program that falls far short of what is needed. This is just a band aid to a deep wound of a problem. Traditionally, Medi-Cal programs have been abstinence-based, so accommodating clients on long acting opioids requires a big shift in their philosophy; despite advances in the research on neuroscience of addiction, programmatic changes can be a long and difficult process. MAT is essentially a harm reduction model, so that’s in conflict with abstinence-based programs.
Long-acting opioids such as Methadone and Suboxone are controversial in that they can be abused or illicitly distributed, but recent advances in injectable buprenorphine (an ingredient in Suboxone) have made these drugs more acceptable. Also controversial is the use of Narcan, a “rescue medication” that some opiate users carry to use along with their drugs as needed. However, even people resuscitated with Narcan from a cardiac arrest, use within hours of their life being saved. Narcan can thus be enabling the maintenance of the drug use.
What do you wish therapists commonly knew about interacting in a helpful way with clients abusing substances?
First, one size does not fit all in treatment. People are different, substances are different, and circumstances are different. Evaluation and treatment planning has to be done on an individual basis.
Second, the client must be assessed throughout the continuum of care, which may take 3-5 years. It is helpful if the client can keep the same case manager throughout the recovery process: one who can advocate for them, be available across facilities, keep progress notes, and as shifts or dips occur, e.g., when an underlying trauma or mood disorder is uncovered. It is important to keep repeating assessments over time. Developing trust for honest communication may take months, and relapses may set back any progress. Keep at it, to really get to know the client and how best to help them.
Third, think beyond the treatment session as far as what structure and support the client in recovery from substance abuse needs. If a person who has been misusing substances 78 hours a week, 1 hour a week of treatment may not be sufficient to make a difference. What happens between sessions is important, and how that milieu is organized. Otherwise prior habits will return too easily. This brings up the potential benefit of easily accessible online communities for support and resources. This low-cost method might offer enough intensity over enough users to save lives. This is quite an exciting prospect I am working on now.
Remember that the person who comes in tomorrow for treatment, may be a terrific mentor to others in need six months from now. Virtual mutual self-help groups, followed by virtual therapy sessions can eliminate the excuse of not being able to get to an in-person meeting.
What do you wish family members commonly knew in order to help their loved one recover?
Concerned family members and friends play a key positive role in recovery. The main things for families to remember are:
- Ask for professional help!
- Realize that this is a family disease: Everyone in the family has been impacted by the substance use one way or another, and should consider seeking professional support as well. Treatment programs generally serve the substance user, not the family.
- There are gaps in treatment support for your loved one, sometimes huge ones, which must be anticipated and planned for. This makes the role of the family crucial both at the front end and “back end” of treatment participation. When a loved one returns from a treatment program, the family may need to rebuild trust and be familiar with recovery issues. The transition to recovery, for the former user, as well as the family takes time.
In summary, what is needed for successful long term recovery for an individual client seeking to move from substance use to sobriety?
Five things are most important for attainment of sobriety:
- Reduce stigma for accessing substance use treatment
- Remember that “one size does not fit all”; The recovery program has to be tailored to fit each client and family, and their needs.
- Create and use the full continuum of care, i.e., detox, residential treatment or sober living, intensive outpatient programs, regular outpatient treatment, mutual self-help groups, and family support.
- The substance use treatment provider community needs to work more collaboratively to facilitate seamless transitions from one phase of treatment to another.
- There is no quick fix. Recovery is a process of learning to be someone different, someone who runs their life completely differently, and this takes time.
What is the San Diego Society of Addiction Professionals (SD-SOAP)?
After working in the recovery field for so many years, I wanted to take my experience and expertise, and play a positive role in “cleaning up” the substance use recovery community (hence the acronym SOAP!). I observed that providers at different levels of treatment were not communicating with each other, and not cross referring even when appropriate to do so. My goal was to set up this idea of a continuum of care. Since there is no one profession which specializes in addiction treatment, it is by nature multi-disciplinary. The conversation needs to include stakeholders as varied as law enforcement officers, nurses, physicians, therapists, families, and employers so that they learn to trust each other and collaborate in the client’s treatment.
Recent statistics show we have approximately 50,000 substance users needing services in our community. We are all affected one way or another by the epidemic of substance use, even when we think we are not. For example, it may be a driver under the influence sharing the road with you. We need to do better!
 Sam Quinones, author of Dreamland: The True Tale of America’s Opiate Epidemic suggests that we, in the U.S., are experiencing a widespread loss of community ties because of the rise of technology, dispersal of the extended family, declining participation in community institutions like organized religion, and economic hardship or general isolation. He posits that this loss of community ties is a critical risk factor for substance use. Do you agree?
Sam Quinones, author of Dreamland: The True Tale of America’s Opiate Epidemic suggests that we, in the U.S., are experiencing a widespread loss of community ties because of the rise of technology, dispersal of the extended family, declining participation in community institutions like organized religion, and economic hardship or general isolation. He posits that this loss of community ties is a critical risk factor for substance use. Do you agree?
I do see the impact of increasing isolation in society. The outpatient treatment setting of Confidential Recovery addresses the needs of professionals with substance use problems who fear losing their jobs or reputation if they take the time off needed to attend residential treatment; this program gives them a new, healing community comprising peers that understand each other and working toward the same goals, and where recovery becomes the lifestyle.
Similarly, at Second Chance, there was a significant effort to create an atmosphere of family /community, and it worked! Interpersonal skills and meaningful relationships are built into “family models” of community living, and peers/staff serve as “substitute family.” The typical stay here can be 9-12 months, which makes it easy to have a stable support system, and from which they could come and go to work. Family activities, like gardening in a community garden and ordinary chores also help facilitate the feeling of community. This is a rehabilitation model; the brain needs time to rewire, so this approach allows that. However, insurance does not cover the cost of necessary life skills training, and that remains a big challenge.
Despite the recent media attention on substance use and new legislation in support of treatment, providers continue to use outdated models that no longer apply to the current state of substance use. This is partly in response to mandates by insurance companies that are not necessarily based on what is best in terms of ensuring a good outcome for a substance using client. 72,000 people died directly from substance use last year; that translates to 10 deaths every hour or 140 a day. That is a staggering statistic.
We all have to start thinking outside the box to address this crisis, and become part of the solution! Please do your part, whatever it is.

Scott H. Silverman is the CEO Founder of Confidential Recovery, San Diego. He was the founder and CEO of Second Chances, a self-sufficiency training program for the homeless and recently released offenders. Scott has been a leader and advocate for clients with substance use for over 33 years in San Diego.
www.confidentialrecovery.com ssilverman@confidentialrecovery.com.
Print a copy of this article here.
What Psychologists Need to Know about ∆9-THC in Recreational Cannabis: Deciphering Science from Spin
By Susan D. Writer, Ph.D.
Recently, before I began a presentation about the science and clinical implications of today’s cannabis, I asked my audience of mental health professionals about their perceptions of recreational cannabis. Some examples of the responses I received included, “I work with a lot of people who say that it helps their migraines, appetite, or insomnia, etc.”; “I don’t see what the big fuss is about; I mean, we’ve had medical marijuana for over a decade”; “It’s no different from alcohol or cigarettes, so if those are legal, why shouldn’t pot be legal too?”; “It’s natural and organic, so it can’t be all that bad for you”; “Marijuana is not as much of a problem as other drugs of abuse because it isn’t as addictive or potent”; “I wouldn’t want my kids using it, but it’s fine for adults who just want to have a good time.” In the group of over 100 clinicians, only a few articulated specific concerns: One addiction treatment provider expressed the concern about increased cannabis addiction (across all ages); another psychologist shared concerns about the adverse effects that marijuana has on symptoms such as rebound anxiety and increased flashbacks in people suffering from anxiety disorders or PTSD, which comprise the majority of his practice; another therapist who works at an inpatient psychiatric hospital expressed concern about the increases in cannabis-induced psychosis that they are seeing at the hospital. What was perhaps most interesting is that the no one in the audience delineated between different types of cannabis or different types of cannabinoid compounds and their differential effects.
I have found through my outreach, educational, and advocacy work in the community, and in concert with other clinicians, academicians, law enforcement professionals, advocacy groups, and judges from across the state of California that the group of clinicians from that presentation, albeit not randomly sampled for a research study, is actually a pretty decent representation of the average Californian’s views and understanding of cannabis and recreational use. This understanding has informed voting, policy, and behavior in recent years. Where do we derive our views, beliefs, and opinions about cannabis use? Is our understanding of cannabis rooted in scientific facts, or is it rooted in “facts” that are delivered to us through savvy marketing campaigns, biased consumers, or industry propaganda?
Let’s start by focusing on some of the specific “facts” which are often debated on social media, in journalism, “fake news,” and across households, as well as some of the aforementioned comments made by colleagues. An internet search on facts about marijuana versus alcohol will yield dozens of hits including images such as the one below.

The websites from which such “facts” are derived will often be well designed and feature testimonials and “science” to support and substantiate their findings.
Before addressing these specific claims, it is important to clarify some of the terminology used in reference to marijuana. The industry has moved toward the use of the term “cannabis” instead of “marijuana”. This, in part, is to help consumers make the association with active cannabinoid compounds that contribute to marijuana’s effects. The flowers, leaves, stems, seeds, and extracts are derived from two plants, Cannabis sativa (plant strains with delta-9 tetrahydrocannabinol (∆9-THC) dominance) and Cannabis indica (plant strains with cannabidiol (CBD) dominance), which contain over 500 chemicals, and over 80 phytocannabinoids that interact with the human endocannabinoid system. . ∆9-THC and CBD are the most widely researched compounds in the cannabis plant; they have similar effects on the body in some areas and opposing effects in others. ∆9-THC has psychoactive properties that cause the “high” experienced by users that increases with potency (CBD does not have these psychoactive characteristics). The increased availability of and risk of psychoactive effects of ∆9-THC is the primary focus of concern among health care professionals. Ultimately, of all of the cannabinoids, ∆9-THC is the compound most associated with addiction, risk, and negative social, psychological, and/or health.
There has been a considerable shift in potency of ∆9-THC available to consumers over the last several decades. The amount of bioavailable ∆9-THC grown in C. sativa plants has increased from 3-5% in the 1960s and 1970s, to 10-12% ∆9-THC by the late 1990s. This statistic applied to both smoked cannabis and cannabis that is used to make baked goods like cookies and brownies. Today, the average amount of ∆9-THC in smoked products is 18-35% (available at any dispensary for both “medicinal” and recreational use), with ∆9-THC levels up to 90%+ in extracts. These extracts are consumed through vaporizers, injections, free-basing, snorting, used in edible baked goods such as gummy bears, brownies, and cookies, or infused in teas, sodas, and alcohol. Even “CBD products” contain as much as 6-12% ∆9-THC to provide a psychoactive effect in addition to whatever effects are experienced from the CBD alone.
It is these implications and ramifications of higher potency that we need to understand as clinicians, consumers, and competent conveyors of information in our community, especially when it comes to intelligently accessing and using cannabis, addressing myths or half-truths, and making comparisons across situations and circumstances.
With regard to comparative research, current NIDA and NIH-funded research on cannabis is strictly controlled with limitations on the amount of ∆9-THC in both cigarettes and bulk cannabis for use with human subjects. Until 2016, the highest available percentage of ∆9-THC available in cigarettes was <8% and the highest available ∆9-THC in bulk cannabis was <10%. In early 2018, NIDA began to release bulk ∆9-THC at 12-14% levels for the use of research in human subjects. The majority of cannabis research conducted prior to 2012 was with a ∆9-THC level of 5% or less, and research findings up until 2016, could only investigate the effect cannabis with 10% ∆9-THC or less. Hence, when marketing representatives and cannabis industry leaders point to the “evidence” from previous research studies that “proves” that cannabis has no deleterious effects on the brain or body, they are citing research that does not evaluate the ∆9-THC levels of the products that they grow, manufacture, or sell. Indeed, there are NO DATA on the effects of the higher, ∆9-THC potency cannabis (in part, because NIDA and NIH have not deemed the higher potency cannabis to be safe to test on human subjects).
Epidemiological data from the California Hospital Association, and San Diego Department of Emergency Management, and San Diego County Health and Human Services Agency’s Medical Examiners’ Office reveal that there has been an increase of 830% in ∆9-THC cannabis-related emergency department admissions in San Diego County between 2006 and 2014 (from 1,108 to 10,302 admissions). In 2016, the San Diego Medical Examiners’ Office reported 462 deaths related to ∆9-THC cannabis. Individuals seek emergency medical attention for cannabis hyperemesis syndrome and cyclical vomiting syndrome (also called scromiting), chest pain, acute cannabis-induced psychosis, panic attacks, tachycardia, respiratory failure, and stroke-like symptoms. Cannabis and cannabis-drug interactions have also been implicated in motor vehicle accidents, suicides, and homicides. These data do not include those seeking treatment for cannabis withdrawal or cannabis addiction.
Referring back to the “fact sheet” in the figure above, it is important to look at the history of two high profile substances that have run the course from panacea to highly problematic. (1) Tobacco cigarettes were initially marketed using physician ‘recommendations’ and testimonials from consumers. Today, the dangerous effects of cigarette smoke are unequivocal. It took 50 years and over 7,000 scientific publications before the Surgeon General put warning labels on tobacco products. (2) When opiates were first introduced into the medical marketplace, they were touted as ‘miracle drugs’ that had little potential for addiction and a low threshold for problematic use or negative consequences; today we have an Opiate Epidemic because of our willingness to blindly trust what an industry was telling us over what our objective eyes were seeing. When individuals began dying from prescription opiate overdoses, those deaths were often as attributed to “respiratory failure” or “heart attack” without any mention of the medication or substance that the deceased had taken The medical community and the public simply did not believe that the average individual could die from prescription opiates and therefore, there was no further inquiry or investigation into cause. The (false) assumption was that an individual who died and happened to have opiates in their system, must have had some underlying health condition which made them vulnerable. Deaths related to prescription opiates continued to be under-reported or unreported for years, not because of an industry cover-up, but because of ignorance and an assumption of “lack of harm.”
There is a sense of déjà vu when it comes to our recent attitude toward cannabis. Can history teach us to be more vigilant? Let’s revisit our chart with some evidence-based edits:

Click here to download a copy of this table.
In conclusion, today’s cannabis isn’t your grandmothers’ marijuana! Cannabis products that are available in the marketplace at dispensaries are far more potent than before and individuals who are using these products are often unaware of what they are purchasing or consuming. The purpose of this article is to give the reader a glimpse of some of the issues that we see in the areas of prevention, intervention, and treatment with cannabis, and what emergency medical providers are experiencing daily in their emergency rooms. Please join us at the SDPA Fall Conference to learn more about the biochemical composition of cannabis and to examine specific clinical ramifications of cannabis intake so that we can competently assess, evaluate, diagnose, and treat, in the context of widespread recreational cannabis use post-legalization in California.

Dr, Writer is the Clinical Education and Public Affairs Officer at Aurora Behavioral Health Care is a clinician, speaker, trainer, and advocate in the areas of mental health and substance use.
Print a copy of this article Writer
The Shadow Epidemic: Why Long-Term Benzodiazepines Cause More Harm than Good
by Shawn Barnes, M.D.
WHAT IF I OFFERED YOU A PILL?
What if I offered you a pill that lowered your risk of Alzheimer’s disease, hip fractures, car accidents, and lung infections? What if this same pill was likely to improve the quality and restfulness of your sleep, increase your daytime energy level, and improve your mood and cognition? No such magical pill exists; however, each of the benefits listed above can be facilitated by getting off benzodiazepines. You may wonder why I am writing about benzodiazepines for readers who do not prescribe or manage medications, i.e., psychologists, social workers, and marriage and family therapists. Psychotherapists, given the frequency with which they see patients, are often in a position to most clearly see how benzodiazepines are affecting a patient’s cognitive or emotional functioning. They may also play a vital role in supporting any patient who makes the decision to get off their benzodiazepine under the close guidance of their physician.
INTRODUCTION
The most commonly used benzodiazepine medications are Xanax, Klonopin, Ativan, Valium, and Restoril. Most patients I encounter have not gone out seeking benzodiazepines, nor are taking them illicitly. In the most likely scenario, the patient was having a difficult month and saw her psychiatrist or primary care doctor, who prescribed Xanax for sleep or anxiety. Five years later, she is still taking Xanax regularly, and is now suffering from cognitive problems, low energy, low mood, or worsening sleep. To my query about what her doctor told her about the risks of Xanax, she says “Only that it can be addictive.” It falls on me now, to have the difficult discussion about the many risks of long-term benzodiazepines, the likelihood that the benzodiazepines are worsening her symptoms, and the complicated process of coming off them.
HISTORY
Before benzodiazepines, we used medications such as Thalidomide, barbiturates, and opium for sleep or anxiety. When benzodiazepines were introduced in the 1960s, they were heralded as a safe and effective alternative, quickly becoming the most prescribed class of medications in the U.S. in the 1970s (Lopez-Munoz et al., 2011). We may look back and roll our eyes at some of the silly and anachronistic indications for benzodiazepines in the 1970s (See Figure 1, for example). However, I would argue that this type of irresponsible advertising set the stage for why benzodiazepines continue to be casually prescribed today for the “treatment” of normal, nonpathological experiences of the human condition. Unfortunately, benzodiazepines have very real, pathological risks.

Figure 1: Valium Ad from the 1970s
THE SHADOW EPIDEMIC
The problems of addiction and overdose from benzodiazepines are well known. The next time you read about a celebrity opioid overdose death, look for a toxicology report. Odds are that he or she was on a benzodiazepine, as in the case of Michael Jackson, Heath Ledger, Prince, Whitney Houston, Tom Petty, etc. Last year, there were over 10,000 overdose deaths involving benzodiazepines (National Institute on Drug Abuse, 2018), yet doctors continue to prescribe them with ever more frequency. Since the mid-1990s, benzodiazepine overdose deaths have increased by about 400%. During that same time, doctors have written 67% more benzodiazepine prescriptions and the strength (in milligrams) of those prescriptions has risen 300% (Bachuber et al., 2016. See Figure 2). The Opioid Epidemic is rightly getting a lot of press and policy attention, but benzodiazepine use is the shadow epidemic. Addiction and overdose are widely acknowledged risks of benzodiazepines, but there are lesser-known, and potentially more serious problems with these medications.
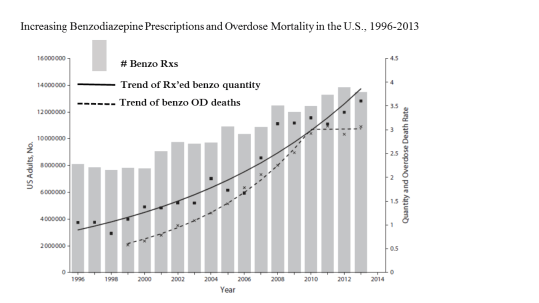
Figure 2 (Modified from Kaufmann et al., 2018)
DEMENTIA
In my clinical experience, some benzodiazepine risks resonate with patients more than others. Patients tend to be less concerned with the prospect of addiction/overdose, because it feels remote and more likely to happen to “someone else.” It’s a shame that addiction/overdose is usually the only risk that doctors discuss with patients, as it tends to give the impression that benzodiazepines are safe, as long as you don’t abuse them. However, in the past decade, mounting evidence indicates that benzodiazepines may increase the risk of Alzheimer’s dementia by 30-80%, depending on dose and length of time exposed (Islam et al., 2016). As we will discuss below, benzodiazepines decrease time in deep-stage sleep. Beta amyloid (the substance that accumulates in neurons and leads to Alzheimer’s) is thought to be cleared from neurons during deep stage sleep (Buscemi et al., 2007). Therefore, one proposed mechanism for the benzodiazepine-Alzheimer’s connection is the accumulation of beta amyloid in neurons by inhibition of deep stage sleep. Of the many risks of benzodiazepines, I find the association with Alzheimer’s disease resonates most with patients. Unfortunately, this risk is seldom mentioned when the prescription is initially offered.
WORSENING SLEEP
Benzodiazepines are powerful sedatives, but tend to worsen overall sleep quality over time. EEG studies have demonstrated that benzodiazepines decrease deep-stage/slow-wave sleep, decrease delta count, increase REM sleep latency, and increase stage 2 non-REM sleep (Poyares et al., 2004), thus resulting in less restful, less restorative sleep. The effect of alcohol on sleep is a good analogy; alcohol works on the GABA neuroreceptor (as do benzodiazepines). GABA modulation (by alcohol or benzodiazepines) can be sedating, but not necessarily followed by a restful, optimal quality sleep. The longer a patient is on benzodiazepines, the more the sleep architecture is disturbed; this is supported by research findings that after patients taper off benzodiazepine, both their subjective and objective sleep quality tend to actually improve (Ashton, 2005)
WORSENING ANXIETY
Clinical data seem to indicate that many people who have been taking benzodiazepines for a long time experience an overall increase of anxiety (Guina & Merrill, 2018). Benzodiazepine users can develop a tolerance for the drug, i.e., they need more medication to get the same anti-anxiety effect after only 4-8 weeks (Bateson, 2002). In addition, benzodiazepines are known to inhibit fear extinction, which is crucial for overcoming anxiety in the long-term. In this way, they can actually hinder recovery from trauma/PTSD and are contraindicated in this condition despite what may be perceived as beneficial effects in the short-term. As with sleep, most people report less anxiety once they have been successfully tapered off long-term benzodiazepines (Ashton, 2005).
OTHER RISKS
In addition to the risks discussed above, long-term benzodiazepines can produce low mood, low daytime energy level, and reduced cognition, often collectively known as “brain fog” (Guina & Merrill, 2018). They are also correlated with higher risks of being in a car accident (Elvik, 2013), falls resulting in hip fractures (Donnelly, et al., 2017), and respiratory infections (Obiora, et al 2013), especially in the elderly.
APPROPRIATE BENZODIAZEPINE USE
As elaborated above, there are many dangers in the long-term use of benzodiazepines, but I would be remiss if I did not mention their benefits when used correctly. Benzodiazepines have an important place in medicine, but their uses are nearly always short-term or intermittent, i.e., not every day, nor for prolonged periods of time. For example, they can be quite helpful for short-term relief from symptoms of alcohol withdrawal, jetlag, specific phobias, or acute anxiety/insomnia. Professional guidelines on prescribing benzodiazepines are clear that they should be used short-term, usually for less than four weeks (Baldwin et al., 2014; Bandelow et al., 2012; Locke et al., 2015; Matheson & Hainer, 2017; Qaseem et al., 2016). However, how many patients have you seen that have been on benzodiazepines for four weeks or less? My guess is not many. Despite these guidelines and the evidence for their long-term adverse effects, 85% of benzodiazepines in the U.S. are prescribed for more than 6 months (Kaufmann et al., 2018). I consider this a public health crisis that, like the opioid epidemic, is primarily the responsibility of physicians. Unfortunately, the American Psychiatric Association has yet to issue guidelines on long-term benzopdiazepine use.
MEDICALLY SUPERVISED BENZODIAZEPINE WITHDRAWAL
We all have patients who have said something akin to, “Wait doc, I know I need to be on Xanax because I once ran out and was off for a few days. My anxiety and insomnia were through the roof! I can’t live life like that. I need my Xanax!” Here the patient is confusing benzodiazepine withdrawal with return of illness, assuming that what they felt during acute withdrawal will be their new baseline. Coming off long-term benzodiazepines can be a profoundly uncomfortable, and medically dangerous, experience. Withdrawal symptoms include intense rebound anxiety/insomnia, hallucinations, depression, heart palpitations, shooting pains, sensitivity to noise and light, suicidal ideation, and seizures (Poyares et al., 2004). The longer a patient is on the medication and the higher the dose, the worse the withdrawal tends to be. Withdrawal from benzodiazepines (unlike other substances) can last for weeks to months, but does wane over time. There are many ways to ease withdrawal, including other medications, herbals, and supplements. Here, I want to emphasize the importance of medical supervision when coming off benzodiazepines. There have been reports of death due to stopping benzodiazepines cold turkey and only a qualified physician, after meeting with a patient and discussing the risks, benefits, and alternatives, should make the decision about whether and how to start the weaning process.
WHAT CAN YOU DO?
As a psychologist or allied mental health professional who conducts psychotherapy, you may understand your patients better than any other health care professional they are seeing. Your patients may trust you and feel more comfortable with you than they do any other health care professional. This provides a safe and supportive space to begin a conversation about what their medication means to them and how they invest themselves in their medication. If a patient has been taking benzodiazepines for years, it would be worthwhile to talk about why they were originally put on it and why they continue to take it. Has their doctor had a full discussion with them about the risks, benefits, and alternatives? Does their doctor keep renewing the prescription without a long-term plan? In my experience, once informed of the risks, benefits, and alternatives, most patients actually want to come off benzodiazepines. Perhaps you can encourage your patient to have an open and honest conversation with their doctor about these issues.
Patients can become physiologically and psychologically dependent on their benzodiazepines, and the topic of re-evaluating their medications should be introduced with skill and sensitivity. As mentioned above, withdrawal from benzodiazepines can be traumatic and a long-drawn-out process; it is vital that they are educated about what to expect and how you can prepare them and support them throughout the process. Your role as a therapist can be invaluable in both encouraging patients to have an honest conversation with their doctor about benzodiazepines, and in facilitating their adjustment to the significant and sometimes scary changes they will experience during and after the withdrawal process. It can be empowering for a patient to achieve a desired and hard-won outcome, and to know that they are able to cope on their own, using their own skills and resources.

Dr. Barnes is an integrative psychiatrist, and has a small, solo practice in Encinitas, Ca. He practices at the intersection of conventional psychiatry, alternative/holistic medicine, and therapy-based approaches. He enjoys having the time to collaborate with therapists and other providers.
Print a copy of this article here.
You Can Do It!: Psychologists as Frontline Providers of Addictive Behaviors Therapy
by Sean House, Ph.D.
“What does it take to be a good addictions counselor?” This is a question I’ve often asked supervisees and students. The simple answer is: BE a good counselor! Many psychologists and allied professionals do not realize that they possess the required skills to help people overcome addictive behaviors; they may assume that a client with an addiction problem needs to be referred to a specialized addiction treatment program, under the misconception that such programs provide a novel treatment that would be different from what they themselves would be able to provide. Certainly, group counseling is a hallmark of residential and intensive outpatient programs. But that’s just a modality of service (and not shown to be any more effective in helping people overcome addictions than individual therapy). The para-professional addictions counselors and graduate-level therapists affiliated with addiction programs, if trained properly, provide various types of psychotherapy. Contemporary treatment programs often advertise that they offer evidence-based therapy such as motivational interviewing, CBT, DBT, EMDR, ACT, and Seeking Safety. In addition, they typically offer some form of family therapy, and various ancillary services like equine therapy or art therapy. Over the past 15-20 years, a commonly used buzzword used when marketing addiction treatment programs is “individualized therapy.”

Artist Unknown (Image from https://scoutingmagazine.org)
Like the title of book by distinguished addictions psychologist, Dr. Tom Horvath, Sex, Drugs, Gambling & Chocolate (2004) indicates, addictive behavior takes many forms. Addiction has very little to do with the drug or activity, and has a whole lot to do with the relationship the person has with that drug or activity. This fact often gets lost in the mainstream conversation about addiction, particularly when the focus is on some form of drug crisis, the current example of which is the Opioid Epidemic. Various drugs take center stage in the news media at different times, and then recede until their time in the limelight returns; examples of these over the years have been methamphetamine, crack cocaine, and marijuana. The problem with focusing on particular drugs is that it puts the focus of attention on the drug, thus demonizing the drug itself, and the solution to the problem takes some form of eradicating the demon (Szasz, 2003). This can take the form of condemning drug sellers (both “pushers” and pharmaceutical companies), trying to prohibit access, and using scare tactics when reporting the dangers of the said drug. These scare tactics continue to be used, even by mental health professionals, with regard to prescribed opiates and benzodiazapines on the one hand, to medicinal or recreational marijuana on the other, often couched in the language of scientific discovery. With so much attention on drugs being the cause of addiction problems, it is no wonder that therapists assume that knowledge about drugs, and some unique way of working with people who have drug problems is required.
Cognitive Surpluses vs. Cognitive Deficits
In cognitive therapy, one way of conceptualizing client’s problems is in terms of cognitive deficits or cognitive surpluses. Cognitive deficits denote a lack of knowledge about a particular phenomenon, as opposed to cognitive surpluses, i.e., having too much knowledge about a phenomenon. This concept applies to therapists’ beliefs about working with clients with addictive behaviors in that many therapists assume they have a cognitive deficit (not having the skills or understanding to work with these people), when in fact they are more likely to have a cognitive surplus (believing that a different set of skills and knowledge then they have is required).
In his magnum opus on the psychological underpinnings of addiction problems, psychodynamically-oriented psychiatrist, Leon Wurmser (1978) goes into great detail about a wide range of psychological problems that create the framework for addiction to exist. [Similar perspectives are highlighted by Kaplan and Wieder in their book, Drugs Don’t Take People, People Take Drugs (1974).]Historical perspectives on addictions treatment underscore the need for addressing the psychological aspects of addiction, i.e., a focus on the person using the drug and not the drug itself, in order to solve the problem. , Miller and Brown (1997) also attempted to shift this balance from cognitive deficits to surpluses by identifying the research that supports why psychologists are well suited to address addictive behaviors with their clients. The bottomline is that if you are a good therapist, you are likely to be a good therapist for clients who have addiction problems.
Do you need to know much about drugs?
The short answer is no. While some knowledge of drug effects, withdrawal effects, and risks of use can be helpful, knowledge of specific drugs and their effects is not central to helping people overcome drug addiction. It is much more important to be a skilled listener, who can get their clients to confide in them their experiences of use, withdrawal, and anxiety about quitting or moderating their use. Understanding the client’s personal experience of drug use and how that has impacted their life from their perspective, i.e., the relationship they have with the drug, is important to understand, in order to help them make changes in that relationship. A client can have different relationships with different drugs, some of them problematic relationships, some, beneficial, and often, mixed.
Personal experience with addiction
The belief that a counselor with personal experience with addiction is better suited to providing addictions counseling continues to persist both in mainstream society and in the helping professions. Indeed, some clients may come to counseling with the belief that a counselor with his or her own history of addiction will understand them better. There is, however, no evidence supporting this belief, or indeed that having a personal history of addiction can yield stronger therapeutic alliances with clients with addictions problems or better treatment outcomes. ,
Having a personal history with addiction can, in fact, complicate the therapeutic relationship; first, the therapist’s experience could have been quite different from client’s, despite superficial similarities in their stories. Second, the assumption that the clients’ experience is so similar to the therapist’s can confound assumptions regarding the client’s level of motivation to change and the goals and tasks from treatment. Over-identifying with the client can lead to countertransference wherein therapists become less effective, due to their personal history. All mental health workers need to be aware of their own countertransference issues as they emerge. Para-professionals may have a lower level of formal training and thus be less familiar with the concept and experience of counntertransference, and how it can manifest in their work with clients. That is not to say that therapists with a history of addiction themselves cannot be good addictions counselors, but that they need to be insightful regarding the boundaries between their own stories and that of their clients’. Therapists without a history of addiction themselves, may be better able to pay attention to their clients’ phenomenological perspective without the constraints of over-identification.
What type of therapy works?
The therapeutic approaches that works to help client overcome addictive behavior is the same ones that facilitate other changes in clients. Different therapeutic modalities and approaches resonate with different clients, and just like in therapy with clients with other problems, therapists must find the ones that best suit what a particular client needs. As captured in the title of Bohart and Tallman’s (1999) book, How Clients Make Therapy Work, it is not what we offer, but what clients do with what we offer.
As a general basis for helping clients through the change process of overcoming addictive behavior, the Transtheoretical/Stages of Change Model proposed by Prochaska et al. (1992) can be instructive in conceptualizing clients’ psychological level of change readiness along with the approaches appropriate to that level. A basic approach would be to use a Motivational Interviewing (Miller & Rollnick, 2013) approach for clients who are ambivalent about changing their behavior, and subsequently using a cognitive behavioral approach to relapse prevention (Marlatt & Gordon 1985) for clients who are actively making behavior change. Research indicates that Motivational Interviewing used tohelping clients resolve their ambivalence about change is enough to put them on track to overcome addiction, without requiring the skills training component of CBT. Psychodynamic approaches may also be effective in helping clients work through the underlying processes that sustain their addiction.

Co-occurring disorders
This is an area in which well-trained and experienced therapists are at a great advantage in helping people with addiction problems. Helping clients to develop and sustain motivation to overcome addictive behavior, and developing the skills to succeed is vitally important. All problems that clients bring to therapy are emotion-based problems (both intrapersonal and interpersonal), and this included addictive behavior. The hallmark of addiction is that it serves to change how the person feels in the moment; typical reasons for engaging in the addictive behavior include wanting to improve a sad or depressed mode, enhance a good mode, avoid withdrawal symptoms, overcome anxiety, and so forth. In each case, it is always a choice that is based on prioritizing current feelings versus consequences, both immediate and long-term.
Given the centrality of emotion in addictions, helping clients with emotional regulation is a key component to relapse prevention. All forms of therapy have ways of helping clients achieve better balance in their emotional regulation. Psychodynamic approaches that address anxiety and defenses, cognitive approaches that teach the connection between beliefs and feelings, behavioral approaches that instruct how behavioral activation affects mode, and humanistic approaches that provide experiential therapeutic opportunities for clients to connect with their feelings in session and develop more tolerance of those feelings.
You Can Do It!
As a good therapist, you know the importance of forming a solid therapeutic alliance with your clients that involves collaborating on the goals and tasks of therapy, and creating a strong bond. These are the same components that are necessary in helping clients overcome addictive behavior and become more psychologically stable. What do you imagine a client’s response would be if you unilaterally determined the goals and tasks for them to change a problem that they aren’t certain they have? Would you expect them to have a strong therapeutic bond with you? Of course not. Yet, traditional addictions counseling has maintained that template. Goals are predetermined (abstinence being the goal expected of all clients who enter most addiction programs). Tasks are predetermined, often involving required attendance at both group counseling sessions and outside support groups. Consequently, the therapeutic bond can be weak when counselors take the opposite of a collaborative approach. With such failure in attending to the importance of the therapeutic alliance, is it any wonder that addiction “treatment” is often not effective ? Therapists who understand the importance of the therapeutic alliance and are willing to work collaboratively with clients, understand clients from their phenomenological frame, and can offer assistance in emotional regulation are in the best position to help people overcome their addictive behavior.
Does that describe your approach to practice ? If so, then you are likely to be an excellent resource for clients seeking recovery from addiction!
References
Bohart, A.C. and Tallman, K. (1999). How clients make therapy work: The process of active self-healing. Washington D.C.: American Psychological Association.
Horvath, A.T. (2004). Sex, drugs, gambling, and chocolate: A workbook for overcoming addictions (2nd ed.). San Luis Obispo, CA: Impact Publishers, Inc.
Kaplan, E.H., and Wieder, H. (1974), Drugs don’t take people, people take drugs. Secaucus, NJ: Lyle Stuart, Inc.
Marlatt, G.A., and Gordon, J.R. (1985). Relapse prevention: Maintenance strategies in the treatment of addictive behaviors. NY: Guildford Press.
Miller, W.R., and Brown, S.A. (1997). Why psychologists should treat drug and alcohol problems. American Psychologist, 52 (12),1269-79.
Miller, W.R., and Rollnick, S. (2013). Motivational interviewing: Helping people change 3rd ed.). NY: Guilford Press.
Prochaska, J.O., DiClemente, C.C., and Norcross, J.C. (1992). In search of how people change: Applications in addictive behavior. American Psychologist, 47 (9), 1102-14.
Szasz, T. (2003). Ceremonial chemistry: The ritual persecution of drugs, addicts, and pushers (Rev. ed.). NY: Syracuse University Press.

Dr. House maintains a private practice, “Addiction & Mental Health Counseling of San Diego,” in the Rancho Bernardo area of San Diego County. Feel free to contact him at sean@addictioncounselingsd.com.
Print a copy of this article here.
Earning Buy-In from Treatment-Resistant Teens
by Lydia Mackeogh, Psy.D.

I have encountered almost every kind of resistant teen in my time as a mental health provider. Some of my favorite and most memorable clients first entered my office scowling, snarling, and proverbially swinging from the chandelier. There is no client quite as rewarding as the one who moves past the outward anger, resentment, and bravado to the underlying fear, sadness, and vulnerability. This journey takes time and patience. It requires a client to actually show up for sessions and to participate fully.
There are special considerations to be made for teens whose primary diagnosis involves a substance use disorder. Addiction alters brain function, attenuates perspective, and impedes judgment. It shapes thoughts and behaviors to ensure its own survival. The patterns of thought and feeling associated with addiction can result in behaviors such as manipulation, false promises, and deception, in order to avoid treatment at any cost.
To make matters worse, the teen may be either under the influence of a substance or experiencing withdrawal from a substance when the subject of treatment is introduced. Their brain is not functioning correctly, they are unable to process the subject objectively, and they slip into survival mode, guided by their addiction. This all but ensures the failure of any attempts to persuade them to accept help.
These treatment-avoidant, self-perpetuating behaviors are not reserved for teens who abuse substances. They may emerge any time a teen wants to maintain destructive behaviors such as self-injury, self-induced isolation triggered by depression, or violent, aggressive outbursts. In order to get a resistant teen to collaborate of their own free will and to help them create real and lasting change, the parent or caregiver must earn some initial currency with them.
In other words, they need to find a way to earn “buy-in” to get their teen to that crucial first session with a therapist. The following are my top recommendations for parents:
- REMEMBER YOU WERE ONCE A TEEN YOURSELF
Close your eyes and remember what you were doing, thinking, and feeling when you were the same age your child is now. Chances are it’s not much different from the headspace they’re in. From a distance, your teenage years might look rosy. But peer deeper into your memories and you’ll remember the fierceness of feeling that accompanied every relationship, the devastating highs and lows that felt completely rational at the time, and the certainty that you were already grown – an adult in an adolescent’s body. You desperately wanted to be treated as such.
You may have experimented with alcohol, drugs, or other risky behaviors yourself. If you did, you may remember exactly what it’s like to seek and try something new or illicit. Today, as a parent, it boils down to making an adjustment on your side: treat your teen as they feel and not how you feel about them. Consider their perspective. It really comes down to empathy; put yourself in their shoes and reflect back to them how it must feel to be them.

Image from NPR.
- SHARE YOUR OWN EXPERIENCES
Openness about your experiences will earn you currency with your teen as quickly as will empathy. Of course, this only works if you’re drawing from similar emotional memories. The content does not need to be identical: for example, your teen may struggle with addiction while you have never experimented with drugs, but if you try hard enough you can certainly relate to wanting to feel good or wanting escape pain. And almost everyone recalls the strong desire to fit in with a group of peers.
If you do indeed have a history of substance use, use your judgment about how much you share, but keep in mind that your teen’s willingness to open up will match yours; if you hold back, they will, too. A good rule of thumb is to discuss feelings rather than facts. Share the difficult emotions you attempted to evade by using drugs or alcohol, without discussing the specifics of what you actually experimented with or the extent of your use. When you do this, you model vulnerability and willingness to be accountable, without handing your teen any justifications for their behavior.
- CHANGE YOUR APPROACH (BECAUSE THIS ONE ISN’T WORKING)
This rubric stands no matter how you’ve been approaching the issue thus far. You may have followed the playbook for perfect parenting. You’ve done all the things the experts advise: you’ve been understanding, you’ve been firm but fair, you’ve set reasonable expectations and described logical outcomes. But if it’s not working, it’s time to try something new. If you’ve been forceful, try being calm. If you’ve been cautious, try being assertive. If you’ve been critical, try taking responsibility for your side of things.
Try exaggerating your sense of your own wrongdoing in the situation. It models accountability for the teen and cues them up to do the same. This may also be the time to confess your own experiences of drinking too much – even as an adult – or share a story about succumbing to peer pressure when you were younger. Remember to share appropriately and avoid sanctioning unwanted behavior in a fit of radical honesty.
- NEGOTIATE AS EQUALS
Approach the topic of entering treatment – or going to that first appointment with a therapist – as if you were trying to find common ground with another adult. Compromise. Consider, or at least make a show of considering their wants and needs. However, remember that you are still their parent and not their friend. Find your line and hold it: every good negotiator goes in knowing exactly where they will and won’t give ground.
For example, don’t compromise by allowing your teen to marijuana in lieu of heroin. Don’t let them convince you they have a problem with pills but drinking beer is no big deal. That’s not good negotiation – that’s you being manipulated. For treatment to work, sobriety needs to be absolute. Not to mention the fact that your urge to be the “cool” parent might earn you a visit from child protective services.
If consensus about treatment eludes you, provide several options. For example, give them three reasonable choices: get assessed for a treatment program or attend five meetings a week or commit to one outpatient therapy session each week for two months. Make it clear that the next step will be one of these options, and the choice is theirs. Make sure the outcomes of reneging are crystal clear, and follow through with the consequences of it comes to that. Negotiations end when you have demonstrated good faith and they have not kept up their end of the bargain.
- BE TRANSPARENT ABOUT YOUR EXPECTATIONS FOR TREATMENT AND/OR THERAPY
When describing the type of treatment that you hope your teen will accept, highlight the positive aspects (e.g., equine therapy! snacks!) but emphasize that there will be therapeutic work to do – and they’re the ones who will have to do that work. If expectations are not clearly laid out, they may feel misled or betrayed. Teens respond to clear expectations, especially when they feel their parents have faith in their ability to meet them. Tell them you have 100% belief in their ability to handle treatment, even if you harbor personal doubts. You may feel a little bit like you have to fake it ‘til [they] make it – but that’s okay.
Many teens with substance use problems say things like, “Do you actually think I’m going to stay sober forever? Do you really think I’m not going to drink and smoke when I go to college?” If this happens, don’t be afraid to acknowledge the legal limits of your influence over their lives. They are right– once they turn eighteen, you can not longer decide what they can or cannot put in their bodies. Make it clear your goal is to help them reach adulthood in the best way you know how—healthy and happy. Your goal is to equip them with good decision-making skills and solid coping mechanisms for handling the ups and downs of adulthood.
- GET SIBLINGS INVOLVED
This one can go either way, but generally speaking, siblings are the Truth-Keepers of Teenland. They know what’s going on because they’ve either seen it themselves or heard it through the social grapevine. This is another example of remembering what it was like to be a teenager: it is almost certain you had secrets from your parents and made daily decisions about what you shared and what you kept to yourself. Siblings also see behaviors that are in plain sight, but which you may not want to or be fully able to acknowledge.
Hiding drugs has now become very easy; they may look like candy, stickers, or flavored vape pens designed for tobacco. Some vape pens – called Juuls – look exactly like a thumb drive, a perfectly legitimate item for a teen to have on them. It can also fairly simple to cheat on drug tests; one can buy fake urine along with a contraption that wraps around the thigh, allowing delivery of the bogus urine to a sample cup. Siblings can be privy to the super-secret world of adolescent special ops, and they can be surprisingly mature in their willingness to speak the truth when they recognize that their siblings and/or friends need help. Also, the teen you are trying to reach is more likely to accept insights or reflections from siblings, friends, or anyone outside the parent-child dynamic.
- PRESENT A UNITED FRONT
This is especially important if you are divorced or separated. It is important to work together in making decisions about your child, and critical that you don’t allow your teen to divert one of you from the mission. The latter is called splitting in the therapy world. Much like the adage “she who has two bosses has none at all,” a teen who gets in trouble probably had a lack of clarity about who was meant to be paying attention. Make sure you are both on the same page about the severity of the problem and the need to take action before broaching the subject of treatment with your teen.
Discuss what drug(s) and how much you think your teen is using. Reach consensus about the ways in which their drug use is affecting their lives, and bring specific, factual examples to your discussions. If you see the problem differently or disagree on the level of care needed, find common ground first: don’t go in undecided or with any degree of ambiguity. Buy-in will be much easier to attain if your child senses that no amount of derailing, manipulation, or other divide-and-conquer tactics will upset your alliance and distract you from your common goal, i.e., getting them in treatment.
- DON’T THREATEN CONSEQUENCES; JUST STATE FACTS
We prefer the word outcomes rather than consequences. Use sentence constructions like “If you choose to do this, it will lead to this.” Examples: “If you continue to smoke weed in my home, you will have your car taken away,” and “If you attend three NA meetings this week, you will earn your car back.” Again, the crucial ingredient with any outcome is follow-through. If you don’t follow through, you lose credibility.
- MODEL SELF-CARE
It is a general rule of thumb that teens are much more likely to do as you do rather than do as you say, especially when your actions don’t match your words. Teens are extremely sensitive to perceived hypocrisy. If you expect your teen to stop doing recreational drugs, then you should stop doing them, too. Same lesson as above: if you tell them to stop smoking weed but you smoke weed yourself, you lose credibility. The current trend in public policy toward marijuana legalization is irrelevant where addiction and substance use disorders are concerned. What is important is to model your own ability to cope with life’s challenges without the need for substances. Adopting a disingenuous zero tolerance policy is counter-productive.
The key is to promote balance and demonstrate a willingness to work on yourself in tandem with your teen. If you model self-care, it increases the chance they’ll do the same. This is particularly true for moms of teenage girls who suffer from anxiety, depression, and low self-esteem, especially if that mom has her own history of struggling with these issues. There’s no better treatment for a teenage girl than to witness her mother taking care of herself, seeing a therapist, hiring a personal trainer, discovering a new hobby, or even just reaching out to friends to socialize or talk through important issues.
- GET TIPS FROM THE PROS
Here are some online resources for parents:
Treatment Spotlight: Family DBT at Evolve
Articles about Motivational Interviewing, an effective technique used in psychotherapy to help the client get more involved in their treatment. MI can be adapted by parents of teens with substance use problems:
Substance Use Resource Center provided by the American Academy of Child & Adolescent Psychiatry.
The SAMHSA Parents and Families page, and this 20-Minute Parent Guide.
Final Thoughts
The essence of getting buy-in from treatment-resistant teens is open, honest, and clear communication that comes from empathy. Your teenager needs to feel heard and understood. You have to be willing to listen to them and adapt your responses to what they give you. You are the adult in the situation, and your word is final. There are certain positions from which you will not and should not budge – but as the adult, it is incumbent upon you to decide what those positions are, at their core, and recognize what types of compromises support versus impede your ultimate goal, i.e., getting your teen the help they need.

Dr. Mackeogh is a clinical psychologist with over fourteen years’ experience in the mental health field. She has worked extensively with people suffering from substance abuse disorders, mood disorders, and problems associated with life transitions, bereavement, and ill health As Program Director of the Intensive Outpatient and Partial Hospitalization Program at EVOLVE in Los Angeles, Dr. Mackeogh is dedicated to working with at-risk youth and providing a safe space for teens who are struggling with life transitions.
Print a copy of this article here.
SMART Recovery®: An Emerging Addiction Recovery Option Worldwide
by A. Tom Horvath, Ph.D., ABPP
Problematic addictive behaviors (substances or activities) are common in psychotherapy clients. In addition to therapy, these clients often benefit from mutual help groups. The most well-known and available group is Alcoholics Anonymous (AA). There are also several dozen similar groups (e.g., Narcotics Anonymous, Cocaine Anonymous), collectively known as 12-step groups. This article presents basic information about another widely available option in San Diego, SMART Recovery.
Finding a mutual help group
The ideal method for choosing mutual help meetings is to sample several, then choose the ones that appear most likely to be helpful. Because of the availability of 12-step meetings, they are typically recommended, sometimes to the exclusion of other options. Many clients are willing to attend a mutual help group, but not 12-step groups specifically. Common objections include that the 12-step program of recovery is oriented around having a belief in a higher power, and that meetings are not conversational.
Nevertheless, there are many advantages to participating in 12-step meetings in general and AA, in particular. These advantages include the high frequency and size of meetings, the large informal 12-step community, the availability of a “sponsor” who will guide a newcomer through the process of using the 12-step approach, and the now scientifically established efficacy of attending AA meetings specifically, if the individual is willing to attend consistently and engage with the AA community (Kelly, 2017). It is worthwhile to review the client’s objections to attending 12-step meetings, to determine if these objections might be overcome. However, many clients will remain unwilling to attend 12-step meetings. Fortunately, other groups are available.
In San Diego, secular groups include SMART Recovery, LifeRing, Women for Sobriety, Moderation Management, and Refuge Recovery. This article will focus on SMART Recovery, which has 60 meetings per week in San Diego County, and has been operating here since 1990.

“Community Affair” (Watercolor by S. Brown Art)
The SMART Recovery organization
SMART Recovery is an international, non-profit organization with meetings in 23 countries. The SMART Recovery Handbook, the primary publication for participants, is available in 14 languages. Currently there are approximately 2,000 community meetings worldwide.
San Diego has one of the largest concentrations of SMART meetings anywhere. There are two San Diego SMART community centers, one in Kearny Mesa and another in Encinitas. In addition to regular meetings, there are also several Family & Friends meetings (SMART’s version of Al-Anon).
The SMART approach
The SMART approach for resolving problematic addictive behavior was recently found to be as effective as three other groups: AA, LifeRing, and Women for Sobriety (Zemore, Lui, Mericle, Hemberg, and Kaskutas, 2018). A review of 25 years of research on AA concluded that “most of the empirically supported mechanisms of AA are found to be more social, cognitive and affective” rather than spiritual (Kelly, 2017, pg. 5). Consequently, we can hypothesize that all mutual help groups base their effectiveness on the same underlying principles. Yalom (1995) suggested that there are 11 common factors in effective groups. These factors may work in both group psychotherapy and mutual help groups: instillation of hope, universality, imparting information, altruism, corrective recapitulation of the primary family group, development of socializing techniques, imitative behaviors, interpersonal learning, group cohesiveness, catharsis, and existential factors.
Although all groups may work by common factors, the surface appeal of addiction recovery groups is diverse. For instance, on the basis of descriptions of SMART Recovery and AA, some individuals may willingly attend one but not the other. Nevertheless, a minority of individuals, in various stages of change, attend both.
SMART supports individuals who wish to stop entirely or limit their problematic addictive behavior, and to pursue a more meaningful, purposeful, and connected life. Rather than relying on a higher power, SMART participants learn SMART ideas and cognitive and behavioral “tools” in order to empower themselves, over time, to act with greater attention to their long-term goals, while not acting on their short-term desires to engage in problematic addictive behavior.
In addition to not insisting on complete abstinence, accepting medication-assisted treatment, and the self-empowering rather than powerlessness orientation, there are several other significant differentiators between SMART and AA. In SMART, there are no sponsors. Individuals desiring a sponsor relationship are encouraged to become involved in AA, instead of or in addition to SMART. In SMART, participants are not required to use the labels “addict” or “alcoholic” (but use of these terms is accepted). In SMART, whether to believe in a higher power, or whether addiction is a disease, or whether moderation of use is a good idea generally, are questions left entirely up to the participant, and not discussed in meetings. SMART’s slogan is “Discover the Power of Choice.”
How SMART meetings operate
In SMART, participants choose their own limits. The meetings focus on how to stay within these limits. Although each participant’s limits may be different, the process of staying within limits (including resisting temptation, advancing self-control, and coping with underlying issues) is common for all. For instance, a participant might choose to abstain from heroin, meth and coke, but smoke pot once a weekend, and have a drink even less frequently. The focus in the meeting is how stay within each of these limits. Participants are also encouraged to identify and pursue other goals. Stopping drinking is more likely to be effective when it is a step in the direction of accomplishing a highly desired goal, rather than simply an end in itself.
SMART offers a set of “tools” for change. These tools would be familiar to any clinician who is familiar with CBT and MI (motivational interviewing).
SMART meetings are primarily conversational, rather than being a sequence of non-interacting monologues as in a 12-step meeting. The typical meeting agenda is a welcome, check-in (around the circle), agenda setting for the discussion period, the discussion period itself (the longest part of the meeting), announcements and pass-the-hat (donations are accepted but there is no charge), and check out. The primary rules are that no one is required to participate, no one can talk too long, the meetings are confidential, the discussion focuses on resolving problematic addictive behavior and related topics, and ideas and suggestions are welcome but advice is not allowed. Meetings are led by facilitators or hosts. Facilitators complete an intensive online course lasting 20-30 hours over eight weeks. Hosts are trained “on the job” in meetings, and a shorter online training course is available.
Scientific investigation of SMART
Scientific investigation of SMART has increased significantly in recent years. The landmark study already mentioned (Zemore et al. 2018), found equivalent efficacy for four different mutual help groups. This finding suggests that ideas like “AA is the only way” or “AA is the best way” are not only inaccurate, but also unhelpful to individuals who prefer to use a different approach.
Penn and Brooks (2000) found that the 12-step and SMART approaches were equally effective in a day treatment setting for chronically mentally ill clients with substance problems. Li, Feiffer, and Strohm (2000) found that 12-step participants had higher external locus of control, whereas SMART participants had higher internal locus of control (until SMART was founded there were few options for individuals approaching addiction recovery from an internal locus of control perspective). Atkins and Hawdon (2007) found that SMART meetings appealed to individuals, and were viewed as meaningful, regardless of their religious or spiritual orientation. Other groups did not have this broad appeal. Blatch, O’Sullivan, Delaney, and Rathbone (2016), in a five-year longitudinal study involving 5,764 Australian prisoners, found a significantly lower rate of reconviction, for inmates who had been involved with SMART, especially among those committing violent crimes. A recent systematic review of SMART identified 12 studies worthy of review (three of them conducted by Alliant doctoral students), and suggested issues to be addressed in future research (Beck et al., 2017).
Recognition of SMART
Recognition of SMART has increased significantly in recent years. Organizations that recognize SMART as an important mutual help option include NIDA, NIAAA, SAMHSA, the National Association of Drug Court Professionals, National Drug Court Institute, Federal Bureau of Prisons, National Institute for Health and Care Excellence (in the UK), Public Health England, Department of Health and Ageing (Australia), and the National Health and Medical Research Council (Australia) (SMART Recovery, 2018).
William White compiled a bibliography of SMART that includes approximately 100 publications (Chaney & White, 2017). The first Surgeon General’s report on addiction, Facing addiction in America: The Surgeon General’s report on alcohol, drugs, and health, mentions SMART as a mutual help option (US Department of Health and Human Services (HHS), Office of the Surgeon General, 2016).
SMART Recovery and multiple pathways of change
Individuals needing to resolve problematic addictive behavior are a highly diverse group. There is no likelihood that any single approach will be effective for most people. Having multiple pathways for change (Fletcher, 2002) increases the odds that an individual will find an appealing and effective pathway. In San Diego there are now enough SMART Recovery meetings to be an easily available option for those interested in attending them.
The national website is www.SMARTRecovery.org
The local website is www.SMARTRecoverySD.org
For professionals or individuals desiring more information about SMART in San Diego, the local website is the place to begin, followed by attending a meeting. Meetings are open to the public. No reservations are necessary.
References
Atkins, Jr., R. G., & Hawdon, J. E. (2007). Religiosity and participation in mutual-aid support groups for addiction. Journal of Substance Abuse Treatment, 33(3), 321-331.
Blatch, C., O’Sullivan, K., Delaney, J. J., & Rathbone, D. (2016). Getting SMART, SMART Recovery programs and reoffending. Journal of Forensic Practice, 18(1), 3-16.
Beck, A.K., Forbes, E., Baker, A., Kelly, P., Deane, F., Shakeshaft, A, Hunt, D., & Kelly, J. (2017). Systematic review of SMART Recovery: Outcomes, process variables, and implications for research. Psychology of Addictive Behaviors, 31(1), 1-20.
Chaney, R., & White, W. (2017). SMART Recovery bibliography.
http://www.williamwhitepapers.com/pr/dlm_uploads/SMART-Recovery-Bibliography.pdf
Fletcher, A. M. (2002). Sober for good: New solutions for drinking problems—advice from those who have succeeded. Plano, TX: Rux Martin/Houghton Mifflin Harcourt,
Kelly, J. F. (2017). Is Alcoholics Anonymous religious, spiritual, neither? Findings from 25 years of mechanisms of behavior change research. Addiction, 112, 929–36.
Li, E. C., Feiffer, C., & Strohm, M. (2000). A pilot study: Locus of control and spiritual beliefs in Alcoholics Anonymous and SMART Recovery members. Addictive Behaviors, 25(4), 633-640.
Penn, P. E., & Brooks, A. J. (2000). Five years, twelve steps, and REBT in the treatment of dual diagnosis. Journal of Rational-Emotive and Cognitive-Behavior Therapy, 18(4), 197-208.
SMART Recovery. (2018) https://www.smartrecovery.org/wp-content/uploads/2018/02/Global-Support-for-SMART-2.pdf. Retrieved 8/20/18.
US Department of Health and Human Services (HHS), Office of the Surgeon General (2016). Facing addiction in America: The Surgeon General’s report on alcohol, drugs, and health. Washington, DC: HHS
Yalom, I. D. (1995). The theory and practice of group psychotherapy (4th ed.). New York: Basic Books.
Zemore, S.E., Lui, C.K., Mericle, A., Hemberg,J., Kaskutas, L.A. (2018). A longitudinal study of the comparative efficacy of Women for Sobriety, LifeRing, SMART Recovery, and 12-step groups for those with AUD. Journal of Substance Abuse Treatment , 88, 18-26

Dr. Horvath has practiced in San Diego since 1983, and specialized in addiction since 1985. He owns and operates Practical Recovery Psychology Group in La Jolla. He has volunteered locally and nationally for SMART Recovery since 1990. He was president of SMART Recovery for 20 years, and continues to serve on the board of directors. He is a past president and fellow of SDPA, a past president of APA Division 50 (Society of Addiction Psychology), and a fellow of the APA and the Association for Behavioral and Cognitive Therapies. He is the author of Sex, Drugs, Gambling & Chocolate: A Workbook for Overcoming Addictions (2nd ed.).
Print a copy of this article here.
President’s Corner

by Cynthia Cotter, Ph.D.
President, San Diego Psychological Association
Welcome to the second issue of The San Diego Psychologist for 2018!
This issue includes articles featuring the presentations from our 2018 SDPA Spring Workshop held this past May 19th, entitled Preparing for the Unthinkable: Mental Health Provider Roles in Disaster Recovery. This was the inaugural event of this title produced by the SDPA Disaster Psychology Committee co-chaired by Deborah Hopper, Ph.D. and Robert McGlenn, Ph.D.; it included remarkable national and local experts in disaster response and was hugely successful. The Committee is currently marketing the event to other organizations and is offering assistance to organizations so that more events of this type might be produced. If you are interested in these efforts, please contact the Disaster Psychology co-chairs. Special thanks to Mary Mulvihill, Ph.D. for being the guest editor of this important issue of The San Diego Psychologist.
We have recently launched our SDPA Fall Conference for this year, which will take place on October 27th, 2018; early bird registration extends to September 30th, so REGISTER NOW! The event entitled, Encountering Substance Use in Clinical Practice: Emerging Issues and Divergent Perspectives focuses on the very timely topic of problematic substance use. There has been a rapid increase in the use of prescription and non-prescription opioid drugs in the U.S. over the last two decades. Drug overdoses have become the leading cause of death of Americans under the age of 50, with two-thirds of those deaths from opioids. Behaviors related to alcohol abuse and alcoholism in the U.S. have also become much more serious. The speaker list for this year’s conference is sterling: Our keynote is George F. Koob, Ph.D., Director of the National Institute on Alcohol Abuse and Alcoholism. Beth D. Darnall, Ph.D., Clinical Professor, Department of Anesthesiology, Stanford University Medical School will present on the dual crises of pain and prescription opioids. We are excited to have investigative journalist Sam Quinones, author of Dreamland: The True Tale of America’s Opiate Epidemic speak on the sociocultural roots of the current opiate crisis. Other topics presented at the conference include marijuana post-legalization, addiction and personality, working with people of color in substance use treatment, support for families of substance users, and understanding relapse. Divergent perspectives on intervention/treatment are presented. There will also bespecial musical presentations. Please join us for our most exciting SDPA Fall Conference to date.
SDPA is pleased to announce that it will be a Platinum Sponsor for the 2018 NLPA (National Latina/o Psychological Association) Conference to be held from October 18th-21st 2018 at the Hyatt Regency La Jolla at Aventine. We are fortunate that this conference is local this year; please don’t miss the opportunity to attend this amazing national event.
If you are already an SDPA member, we are so happy for your participation. If you are not, there is no better time to become a member. Members receive many benefits and discounts, including lower registration fees to the 2018 SDPA Fall Conference. Join SDPA NOW! We hope to see you soon.
Editorial
The San Diego Psychologist is grateful to Dr. Mary Mulvihill of the SDPA for guest editing this important issue based on the SDPA Spring Workshop entitled, “Preparing for the Unthinkable: Mental Health Provider Roles in Disaster Recovery.” She was responsible for curating the content, gathering and writing the transcripts, and doing the initial edits for this issue. She has written the Editorial for this issue.
The featured articles in this issue are not verbatim transcriptions of the authors’ presentations. The transcriptions have been edited for content, length, copy, and grammar for the purposes of this publication.
Please give us your feedback in the comments section of this or the other articles in this issue, and as always, thank you for reading.
Gauri Savla, Ph.D., Editor, The San Diego Psychologist





Dear Readers,
The San Diego community is on the leading edge of disaster response. In 1984, a McDonald’s restaurant in San Ysidro, a border town in San Diego was the scene of one of the earliest mass shooting incidents in our country’s recent history. Twenty-three people, including many children, were killed by an active shooter. This incident caught the Disaster Response community completely off guard, since mass shootings were rare at the time. After careful study of the emergency response to the event, ways to minimize casualties in similar events were devised in order to increase readiness. Some of the changes instituted included having SWAT teams carry their weapons with them in their vehicles for faster response, and developing robots to retrieve the wounded from the disaster site when unsafe for medics to do so. These “lessons learned” were applied nationwide to different extents, but particularly here in San Diego, where a shocked and saddened community took the need for improved disaster response seriously. Every disaster, although unwelcome and terrible, is an opportunity to study potential challenges and find ways to anticipate and solve them when the next disaster occurs.
The lessons learned from this and other incidents that followed have informed the “best practices” in the field of mental health disaster response field. The current issue of the San Diego Psychologist highlights the program from the SDPA 2018 Spring Workshop, Preparing for the Unthinkable: Mental Health Provider Roles in Disaster Recovery. The goal of the workshop (and this issue of The San Diego Psychologist) is to help you understand how the local San Diego County disaster response system works, where you fit in, and how you can help as mental health professionals.
The workshop was carefully planned and executed over 18 months by the Chair of the invaluable SDPA Disaster Psychology Committee, Dr. Deb Hopper and her team, which included SDPA members, Dr. Bob McGlenn, Dr. Glenn Lipson, Dr. Wendy Tayer, and Mr. Bo Robertson. Based on their knowledge of the field, they determined the agenda and assembled a first-rate team of speakers. They were also integral to the preparation of this issue of The San Diego Psychologist.
The conference, held on May 19th, 2018 at West Auditorium at Scripps Mercy Hospital was a tremendous success, attended by 90 mental health professionals and graduate students. The dynamic speakers, all experts in the field of Disaster Response, were led by keynote speakers, Drs. Chip Schreiber and Melissa Brymer. All speakers had extensive, first-hand experience on the front lines of many recent local and national disasters.
Dr. Schreiber is one of the nation’s leading “second responders,” i.e., the mental health professionals participating in the recovery efforts on site. Dr. Brymer was the lead mental health professional in the 5-year post-Sandy Hook school shooting recovery effort, as well as many other school and workplace shootings across the country. She also worked with Dr. McGlenn as a second responder after the shooting at Santana High School in Santee, in 2001.
From our local resources, Ms. Crawford, head of San Diego County’s Emergency Response Command Center, is the one who takes command instantly when local disasters strike. She is capable and knowledgeable, and we were fortunate to hear her speak at the workshop. Dr. Lipson has extensive experience in our local Red Cross shelters and shared many tips about what to expect and what is most helpful in the immediate days after an event. Dr. Tayer applies the CBT model to explain why people do what they do when challenged by a disaster and the pitfalls of stress-induced, maladaptive thinking that one must be aware of. Dr. Hopper shared excellent, pragmatic tips on how to prepare for a disaster and cope when the “unthinkable” happens, both at home and work, including with our clients.
If you were not able to attend the event or if you just want to review some of the informative training provided, this issue of The San Diego Psychologist is for you. Through this issue, the experts in the mental health disaster preparedness field, will answer many of your questions about how you can prepare yourself, your family and your practice for the “unthinkable”.
We hope that you will be inspired to take a leadership role in your own community to help prepare and if needed, respond, when your mental health skills and expertise are called for.
Please refer to the list of Resources, compiled by the SDPA Disaster Psychology Committee, for additional, up-to-date disaster preparation and response information and the list of local mental health-related disaster response organizations, should you be inspired to consider the volunteering options available to mental health professionals.
Mental health professionals play a vital role Disaster Preparedness, Response and Recovery – be part of the solution!

Mary Mulvihill Ph.D.
SDSU Graduate School of Public Health
Guest Editor, Disaster Preparedness Issue of The San Diego Psychologist
