Category: 2017
President’s Corner
by Annette Conway, Psy.D.
It has been an honor and privilege to have served as the 2017 President of the San Diego Psychological Association. I can say with conviction that this has been one of the most rewarding experiences of my professional life, and one that seemed to begin and end in the blink of an eye. I extend my gratitude to the current and past Board members for their consistent support and encouragement.
In this year, we continued the tradition of the SDPA to host important events and meetings for the benefit of our members and the community at large. Together, we hosted the highly successful Fall Conference, that that received recognition throughout the San Diego psychological community, held several networking and social opportunities at no or little cost to the members, educated the public with 30 committees and task forces, collaborated with other professional organizations such as San Diego CAMFT, the Psychiatric Society, UCSD, and the San Diego Academy of Child and Adolescent Psychiatry. We also sponsored and co-sponsored nine Continuing Education courses.

Credit: Instagram
We established a new, user-friendly website complete with a comprehensive member referral directory, and continued to implement the structural re-organization of the Board of Directors and office staff. We improved the fiscal statements and increased the bookkeeper’s role, thus providing better overall financial documentation.
I am especially pleased to report that we received the Award for Outstanding Chapter from the California Psychological Association this year. Our advocacy efforts remain strong; the Government Affairs Committee engaged in several proactive events in support of the California Psychological Association by participating in the Leadership and Advocacy Conference in Sacramento, contributing financially to the Political Action Committee (PAC), and by hosting a legislative Meet and Greet in San Diego.
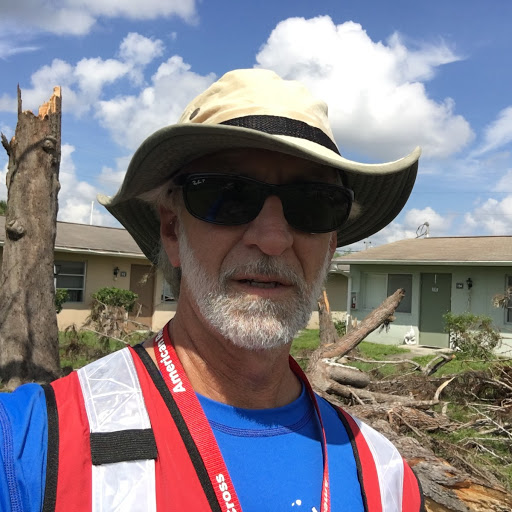
It is an important time for our Association as we continue to adapt and grow in this period of global change. The Disaster Psychology Committee’s collaboration with the Red Cross in responding to the mental health needs of residents in Houston, Mexico, Florida, Puerto Rico will continue to thrive and educate the mental health community as well as the public about how to care for themselves and others before, during and after disasters. In this last issue of 2017, the San Diego Psychologist highlights some of this important work conducted by our intrepid colleagues.
With the help of you, our members, we have accomplished our most important goal this year, i.e., to actualize the SDPA Mission Statement, “To create a community for psychologists, to promote the profession of psychology, and to serve the public.”
I am excited for Dr. Cindy Cotter and her 2018 Board of Directors, and know that with your ongoing support, they will take SDPA to even greater heights. Best wishes for a successful year!

Dr. Conway is a clinical psychologist in private practice and the President of the San Diego Psychological Association.
Editorial
“Are you the sort of person who gloats when they see a woman fall, or the kind that celebrates a magnificent recovery?” (J.K. Rowling)
2017 has been quite a year. Besides the ongoing aftermath of the 2016 elections, it has been a record-setting year for relentless, devastating natural disasters in our country, ending with the massive wildfire outbreaks first in Northern California and presently, much closer to home. As the Thomas Fire continues to ravage areas north of Los Angeles, I cannot seem to shake the sense of foreboding for the future of our planet. Even as we deal with the obvious physical losses from these events, the psychological toll they take can often be overlooked. It is safe to say that our role as mental health professionals has never been more vital to disaster relief efforts than it is today. We are among the privileged few who witness the remarkable resilience of the human spirit in our work with victims of disasters. This last issue of the year, themed “Disaster Psychology,” features three articles focusing on the role of psychologists and allied professionals in the recovery efforts aimed at mitigating the fallout from disastrous events.

The Rebuilding of a Heart by Gayle Madeira, 2005
Dr. Stevens has written a poignant narrative about his first-time experience working as a Red Cross volunteer; his descriptions of the damage caused by Hurricane Irma and his work in aiding and supporting the victims paint a vivid picture. Dr. Tayer’s article on her experiences as a CERT volunteer is full of valuable information on how you, as a citizen, can help in local disaster relief efforts with confidence and competence. Finally, Dr. Hopper’s article on building resilience and self-care should be required reading for all mental health professionals; we need to be resilient and emotionally well ourselves in order to care for our patients as well as our family, friends, and colleagues. I am particularly proud of this timely issue, and I hope you learn greatly from these thoughtfully written pieces.
I want to close by expressing my gratitude to Dr. Annette Conway for her kind words of encouragement and support through this year. I am delighted to continue as the Editor of the San Diego Psychologist through 2018 with Dr. Cindy Cotter at the helm of the SDPA.
Thank you for your continued support and readership. I look forward to receiving your contributions to future issues of the Newsletter.
Happy and peaceful holidays to all, and best wishes for the new year; may it be a far less tumultuous one.

Dr. Savla’s private practice in Encinitas, CA is mainly focused on seniors with aging-related challenges and/or mental illness. Before devoting her professional life to clinical service, she studied primary psychotic disorders among older adults at the University of California, San Diego and the VA San Diego Healthcare System. She has co-authored 30 peer-reviewed papers and book chapters to date. She has been the Editor of the San Diego Psychologist since 2016.
Hurricane Irma: Notes from the Field
An Eyewitness Account of a First Time, Red Cross Disaster Volunteer
by Mark W. Stevens, Ph.D.
Soon after Hurricane Harvey hit Texas in August, 2017, I came across the memo from the California Psychological Association (CPA) for mental health professionals to volunteer services for disaster relief efforts. These efforts were via the Red Cross, and as I mulled over teaming up with an organization with so much negative press, Hurricane Irma was barreling straight for southern Florida, promising to grow into a potentially catastrophic level 4 or 5 event. After much contemplation, and with encouragement from my wife, I decided to find out for myself what the Red Cross was about. My rationale was that regardless of whether the Red Cross was good or bad, it was the only means by which I could help as many people as possible in the moment of this terrible crisis; I figured that by experiencing the workings of the Red Cross firsthand, I could also offer constructive criticism, if I had any.
After contacting the Red Cross in San Diego, I completed an on-line application and submitted to a background check. I underwent extensive on-line training, some of which was focused on “psychological first aid” aimed at providing mental health disaster relief services. I completed these preparations in the evenings and over two weekends while maintaining regular client appointments and preparing my clients for my absence upon deployment to one of the disaster sites.
On Friday, Sept 15th, 2017, I was notified that the Red Cross needed my services in Orlando, Florida. The San Diego headquarters of the Red Cross connected me to a service that arranged my flight, and issued my vest, ID badge, and a Red Cross prepaid expense card. I learned that the Red Cross was concurrently active in 67 other disaster situations such as fires and floods across the country, in addition to hundreds of international crises, including the earthquake that had just ravaged Mexico. Things were becoming very real and in a rare moment of self-doubt, I honestly wondered what I had gotten myself into.

I flew out the next day, fully aware that this was going to be a seminal event in my 20 years in practice as a clinical psychologist. Upon landing, I met up with a fellow volunteer and Red Cross veteran named David, and together, we made our way to our assigned hotel for the night. The next day, Dave and I, along with a hundred-plus other veterans and first-timers made our way to the staging location to receive our orientation and assignments. A Disaster Mental Health orientation was given by Dr. Bill Martin, the lead person for the mental health volunteers, and several of us were assigned to a shelter in the town of Estero, located along the Gulf coast in Lee County, roughly five hours southwest of Orlando. We were greeted by Peggy, our Disaster Mental Health supervisor and taken around the shelter to meet with its roughly 400 residents. It was late, and this mass of men, women, and children had already done what they could to make a temporary home for themselves on cots in a large gymnasium. The other volunteers and I spent that evening sleeping on our own cots in the communal staff room at the shelter.
The next day, we were each teamed up with a partner for the duration of our deployment. I had the good fortune of being teamed with Ellen, a marriage and family therapist from North Carolina; this was her second Red Cross deployment. Ellen and I spent the morning conducting mental health interventions with shelter residents, and were then reassigned to another shelter in North Fort Meyers, where we began conducting interventions with both shelter residents and the staff, comprising volunteer nurses, police, and various other disaster action team members. We learned quickly not to get too settled in any one place as our assignments were likely to vary on a daily or even hourly basis.


The North Fort Meyers shelter was inhabited by residents under unusually severe duress. Many had been homeless even before Irma struck; some were suffering from severe mental illness and had been without their medication for days. Other residents had lost homes, cars, and jobs as a result of Irma, and some had been separated from or lost contact with family members. As the Red Cross was actively engaged in the Response phase of Disaster Relief, its primary objective was to move everyone, especially the most vulnerable, to a safe place.The experience of emotional duress was not exclusive to the residents; staff volunteers and management alike struggled with the immensity of the chaos, overwhelming need, and long hours demanded of them to ameliorate the suffering created by Irma. Ellen and I spent an entire day conducting interventions among staff and residents. That evening, all disaster responders, Ellen and I included, were assigned lodging at the Marriot Resort on Marco Island in Collier County.
The beauty of this luxury venue was strangely juxtaposed with the no-frills grit of its current residents – the volunteers belonging to various disaster response teams, all decked out in their respective distinguishing garb. Such juxtapositions were ubiquitous in Southern Florida; the devastation, which was so profound that in many places the debris piled up along the roadsides was high enough to block my view of the homes behind it; dozens of buzzards (yes, buzzards!) circling overhead, underscoring the loss of animal life. These scenes of despair were in sharp contrast to the tenacity of the people and the intense recovery efforts as evidenced by work trucks for every kind of outreach program, repair, or reconstruction job lining the highways for as far as the eye could see in either direction, with crews working around the clock along the highways.
The needs of the residents, the relief operation, and indeed, the Disaster Response personnel were constantly changing. Two days after working at the Marriot, Ellen and I participated in a large media event with other volunteers from the Red Cross and other agencies, such as the Salvation Army, local support and outreach groups, churches, FEMA, insurance companies, and interns working for the United States Senator from Florida, Marco Rubio. During this day-long event, we provided information and resources to a continuous line of people desperate for help—one person after the other, family after family, broken, frightened, and confused, with needs ranging from the very basic (such as food and water), to resources for repairing and rebuilding their homes, finding jobs, and securing cleaning supplies for the mold, rats, and other infestations that are part and parcel of a post-disaster world.


On September 21st, Ellen and I returned to the North Fort Meyers shelter where we resumed our work assessing and helping both residents and staff take a few steps closer to a state of overall health and well-being. There were a few particularly memorable residents that left a deep impression on me. One was a man who had been living in Colorado with his wife prior to hurricane Irma, and flew to Florida on their proverbial “last dime” for the promise of a new and much needed job. Shortly after arriving, Irma struck and destroyed the business and any hope he had of employment. Another was a 94-year old woman whose home was destroyed in the storm. She had lost contact with her daughter and son, and we were working to help her get out of the shelter and into a temporary assisted living situation. She had a hard time processing why she couldn’t go home, and why her children weren’t there to help her. It was clear that both cases would need a prolonged recovery effort that would long outlast my own deployment.
Many of the mental health volunteers were interested working directly in the community and on Friday, September 22nd, Ellen and I were assigned to follow a Red Cross Emergency Response Vehicle (ERV) into Lehigh Acres, one of the harder hit neighborhoods. As we pulled into the area, it looked like a ghost town with very few people out and about. While the ERV staff blasted the alert horn and announced their presence via loudspeaker, Ellen and I split up and walked through the devastated neighborhood in search of the homebound. We wound our way around the broken homes, fallen power lines, snapped trees, and dead vegetation, and eventually found our way to the community center, where the facilitator lent us one of the center’s golf carts to make our job easier. The temperature was in the 90s with humidity to match, and the residents had been without power until the day before we arrived.

The following day would be the end of our nine-day deployment before we would fly home. Ellen and I decided to spend our last full day working in the neighborhood of Golden Gate, located just north of Naples in Collier County. We were told that the devastation there may actually surpass any we had seen elsewhere. The eye of hurricane Irma passed directly over this town causing flooding and spawning tornados. Given our experience in Lehigh Acres, we decided to head to the community centers in order to gather more information and assistance for our efforts. There were signs of devastation everywhere; the residents were still without power, there was visible flood damage everywhere, and many homes had roofs missing, ceilings caved in, and walls crumbled to rubble.
We spotted a FEMA truck parked in front of the center and we spoke to the people staffing it. They were ready to move on as they had been there for a while and as yet had seen no residents. But Ellen would not hear of it; she asked them if they would give us a couple of hours to round up some people. The FEMA staff agreed, but we had a challenge ahead of us: the area was sprawling and we didn’t know where best to go. Then, as luck would have it, we met a volunteer who led us to a trailer park in the center of it all. The residents, mostly Hispanic, were lining up as we arrived for food being passed out by a local Christian group. Neither Ellen nor I speak fluent Spanish, but language was no barrier when Ellen waved one of the many donated Mickey Mouse toys that we had in the car, which prompted the kids to come running toward us, and their parents followed. In an instant we were surrounded, and eventually made our way to the pastor of the Christian group who announced the purpose of our visit over a loud speaker. English speakers in the community then guided us to those they knew were in greater need and more reticent to seek help on their own. One inspirational member of this community was a man named David, who despite being disabled himself, cared for his mother in their modest trailer. David appeared to be the de-facto counselor in his community and was doing everything he could to help his neighbors. We were particularly impressed by his awareness of the importance of his own well-being, apparent when he would catch himself revving up emotionally, and without skipping a beat would say out loud to himself, “Relax!,” and continue with whatever he was saying or doing.
The day was hot and humid as they had all been, and we were tiring rapidly. In addition to providing the community with information regarding how and where to obtain food, water, clean up kits, and the possibility of financial assistance, we offered a compassionate ear and encouraged self care. We had passed on the information about locating the FEMA truck, but worried that the needs of these people far surpassed what we could do for them. Our hope was that a Red Cross ERV would show up with much needed supplies. As we made our way back to our car, another Christian group had arrived to help the community. We advised them of some of the need we encountered, and just as we were about to leave, a rental truck pulled into the area, driven by a man wearing a Red Cross vest. That was a huge relief; the volunteers of the Christian group joined us in handing out food, water, clean up kits, roof tarps, diapers, rakes, shovels, etc. to the residents.
Returning to the community center, we saw that the FEMA personnel had set up camp, and a line of residents was waiting to talk with them. We set up a table in another area, and asked FEMA to direct to us anyone who could benefit from our assistance. After roughly another hour of seeing relatively few people, we checked the FEMA room again. It was packed! Observing that people were finally getting their immediate concerns addressed, we decided to leave. We’d like to think our efforts that day in the community had at least a little to do with this successful outcome.
Suddenly, Saturday evening had arrived, and the next day I would be flying back home to San Diego, California, and my partner to North Carolina. I say suddenly, because for nearly the entire nine-day deployment, I was living in an altered state of reality with very little sense of time. I worried prior to deploying, how I would handle a disaster situation, and now I wondered how I was going to handle returning to a more orderly life where any needs and wants could be readily met. Odd as that sounds, please consider this: while much of the rest of the country was bickering over whether it is appropriate that an athlete “take a knee” during a playing of the national anthem, or whether entertainers should be boycotted for pointing out the flaws in our country, and discussions about race, ethnicity, gender, sexual orientation, politics, religion, age abound, the people I had encountered in the place I was preparing to leave were truly concerned with the well-being of others. Both staff and residents worked harmoniously together, with little regard for socio-cultural differences, their singular goal to help their fellow man or woman get back on their own feet. Having been in the throes of disaster recovery, I have seen firsthand the hope, determination, and resilience that humans are capable of.
Ellen asked me several times if I would consider volunteering again; my answer was always, and still is an unequivocal yes. And I know she feels exactly the same. We know we did everything we could to help those in need, but what we received in return far surpassed anything we gave. The work was hard, but everywhere we went, we met and worked with selfless people, whose focus was the welfare of others, including us. The attitude and the energy of both were incredibly and unusually positive for the most part, especially considering the circumstances. It was focused on moving forward.
With regard to the Red Cross, I have never experienced a more single-mindedly determined group of people, collectively or individually, whose sole mission was to help those in need at such a deep level. One veteran Red Cross volunteer we encountered was a 74-year old woman with unparalleled energy and dedication; after wrapping up her work in Florida, she was making arrangements to fly to Puerto Rico to help the victims of Hurricane Maria. Like any large organization, the Red Cross is far from perfect and the criticisms and complaints directed toward it are not always unwarranted; but having been in the trenches with them and seeing the remarkable work they do, I can’t help but wonder how many people would suffer and potentially die if it wasn’t for their efforts.
Last but not least, I would like to acknowledge my unexpected pleasure of meeting and befriending Ellen, just one of the many incredibly strong and focused individuals I met during my experience in Florida. Her heart of compassion and empathy helped me to maintain my bearings on a daily basis. Working with her inspired me to work at a higher level than I thought I could. I look forward to continuing this friendship for many years to come.
Print a copy of this article here.
Dr. Stevens is a clinical psychologist, and currently has a private practice in Poway, California. He has previously practiced in Hawaii. He is married and has six daughters. When not working, he enjoys music, hiking with his wife, painting and drawing, and writing short stories, poems, and novels.
CERT
by Wendy Tayer, Ph.D.
CERT stands for Community Emergency Response Team and is a national FEMA program designed to train ordinary citizens to help first responders in their own communities. I became aware of the program when I attended an “Are You Ready” presentation at my local library presented by local CERT members who were fellow school moms. I felt inspired. It was 2014 and I had more time on my hands because my youngest child had recently passed his road test. With the lion’s share of day-to-day parenting behind me, I was looking to expand my horizons to community-minded activities beyond the PTA and education foundation volunteer positions.
I had lived through several fires and the countywide blackout in San Diego, the London Tube and bus bombings of 2005, and lost a high school friend in the Twin Towers on 9/11. I decided that it was time for me to extend my skills as a clinical psychologist and a caring human being to everyday life outside of my psychotherapy office. International, national and local events in the past 15 years had heightened my awareness of the critical importance of learning survival skills.
I called the phone number that was listed in the small article in my local newspaper and registered for the next CERT academy at my local fire station. I found myself among a variety of North County citizens much like one might find during jury selection – various ages, backgrounds, ethnicities and reasons for seeking the training. The one quality that we shared was the desire to help others and to learn adaptive coping skills in order to do so. My academy training was concise and feasible for working professionals, comprising two weekday evenings and three Saturdays. The training modules include:
>>Disaster Preparation
>>Medical/Basic First Aid Training
>>CERT organization
>>Disaster Psychology, Terrorism
>>Fire Safety
>>Cribbing (technique for using materials on hand to lift heavy debris in order to free people and animals who are trapped), and
>>Light Search and Rescue.
The course ended with a final drill/practice session. CERT instructors and local firemen lead the training sessions and drills at local firehouses.

“You are Not Alone” Art by DanSun
In the past year, FEMA added a mandatory online course which consists of a 6 hours of comprehensive CERT material on the FEMA website. Course content includes similar material in addition to an overview of CERT, detection and management of hazardous materials, incident command/ communication protocols during a disaster, and the ubiquitous multiple choice test at the end. CERT typically holds two academies per year over San Diego County and offers other informational sessions on disaster related topics throughout the year such as swift water rescue, use of search and rescue dogs, earthquake preparedness, and operation of ham radios for use when cell phone and/or landlines are down. CERT San Diego organizes a countywide drill every year which varies in location and type of disaster that is simulated. Throughout the calendar year, regular rehearsal of CERT skills is emphasized. All graduates of the program become certified, receive an official CERT ID card and a GO BAG which is stocked with supplies for use in the event of a disaster. Typical contents include first aid supplies, flashlight, work gloves, hard hat, official CERT vest, colored tape for identifying victims of a disaster by type of injury, markers for keeping track of victim transport as well as search and rescue missions. Certification is valid for two years and recertification is accomplished by retaking the online course and attending the last day of a local academy in which the skills are put into practice and rehearsed in a simulated exercise. Alternatively, members may participate in the countywide drill for credit. Both experiences are worthwhile, and offer valuable opportunities to keep current with one’s skill set.
CERT also plans and implements drills during the California Shakeout in October and for Biohazard disasters such as a countywide anthrax attack. I find these drills instructive and reassuring; I now know that the county is prepared with a stockpile of antibiotic treatment doses to counteract anthrax or another biohazard for the entire population of our county. There are plans in place for administering the doses to the populace in a very organized, efficient fashion. CERT was initiated in San Diego following the 2003 Cedar Fire when it became clear that first responders cannot be everywhere when wide-ranging disasters strike. Furthermore, infrastructure and communications systems can be damaged, which delays the actions of first responders. The rationale for CERT is that the people who are in the immediate vicinity of the event can be trained to respond to the event and can save lives, extinguish fires, find missing persons, and administer emotional first aid while waiting for firemen and emergency medical personnel to arrive. CERT provides opportunities for citizens to play a role in helping to diminish the impact of the disaster to affected persons in the immediate aftermath of such events.
CERT encourages each member to play a role in which he or she is comfortable. There are many CERT roles, including incident commander, scribe (note taker), first aid/triage worker, search and rescue team, and record keeper outside of a building to count bodies removed, among others. Members are given the choice to perform a duty that they feel competent to do at a drill or actual disaster site. It is very important to note that CERT members MUST be activated by local first responders or CERT personnel in order to perform CERT functions during a disaster. Activation usually happens via a cell phone call or text. I have never been activated during an emergency. But I have had multiple opportunities to rehearse my skills. As a psychologist, I have taken the opportunity to become an expert in Emotional First Aid and have taught the mini course to local CERT members. I have also passed on some of my training to my graduate students as I believe that it is important for them to have the knowledge that these programs exist. That way they know how to get involved should they be interested. I strongly feel that as mental health professionals, we be armed with survival skills to apply in our personal and professional lives.
The Emotional First Aid mini course consists of teaching CERT members (not just mental health professionals) the fundamentals of disaster psychology – describing a typical disaster scene, the array of symptoms that people can experience in response to trauma/disaster, how to talk to disaster survivors, basic empathy training, how to approach and aid individuals with special needs (seniors, mentally ill, blind, dementia, autism, etc.) in addition to practical coping approaches, education about resiliency and self-care, utilization of the CERT team for relief and breaks, debriefing after a disaster or drill and useful apps for survivors and CERT members to utilize that may help with coping, finding loved ones, and locating a temporary shelter. It is a lot of information, but generally well-received by my CERT audience.
CERT members are not limited to disaster related duties and services. They are also encouraged to assist with community safety projects and help friends, coworkers and neighbors make preparations for emergencies (The “Are You Ready?” presentation that initially inspired me was one such community safety project). Examples of readiness for individuals are education about mitigating disaster in the home by removing potentially hazardous or flammable materials, assessing one’s property and workplace for unsecured objects in the event of an earthquake or ensuring that one’s house has a fire resistant roof and property is clear of dry brush and vegetation, organizing and updating a family Go-Bag, and volunteering at local public events to educate the public about CERT.
CERT is one of many ways to get involved with disaster recovery, and the array of disaster related organizations can be confusing to navigate. CERT is unique and distinct from the Red Cross, the most widely recognized disaster response agency in the world, in that the former is a federally financed FEMA program in which citizens help out when disasters occur in their own neighborhoods. The Red Cross is an international humanitarian organization that provides emergency assistance, disaster relief and education in countries around the world. The American Red Cross (ARC), a subgroup of the international agency, deploys volunteers locally and domestically at disaster sites all over the United States. The ARC focuses on meeting basic human needs such as shelter, food, and mental health services (psychological first aid), but does not provide medical or search and rescue services. In contrast, CERT trains its members in basic first aid and search and rescue techniques as well as psychological first aid but does not provide shelter services, per se. However, CERT members may undergo specialized training to become certified shelter workers. There are opportunities for the two agencies to collaborate and efforts are underway to foster more teamwork between CERT and ARC in San Diego County.
CERT training and membership has been an extremely rewarding and enlightening venture for me over the past three years. I have learned a great deal, and feel confident that I know how to act in the event of an emergency (the latter is a testament of the adeptness of the CERT program in training its members to perform their skills in the event of an emergency). It emphasizes teamwork and self-care above all else. A major drawback of the program is that CERT does not do much to actively recruit new members despite being always in need of new members as existing members age out or retire from the program. It relies on word-of-mouth communications, booths at local street fairs, and local newspaper listings to advertise their academies. These efforts pale in comparison to other agencies that use the internet and social media to their advantage. One or two CERT groups have their own apps for operational purposes, but a universal app developed for use all over the country would be welcome. There are opportunities to express concerns such as these at local meetings as CERT prioritizes a team approach and clear communication.
In conclusion, I urge you to consider CERT training if you are interested in extending your helping hands to the outside world beyond your office. The world events of the past few years suggest that it is critical for us to be trained in disaster preparedness, both in our personal and professional lives.
Feel free to contact me with any questions at wtayer@ucsd.edu.
For more home preparedness information, you can access ARE YOU READY? at www.ready.gov.
For more information about CERT San Diego, go to www.sandiegocounty.gov/oes/community/oes_jl_CERT.html
Print a copy of this article here.

Dr. Wendy Tayer has been a clinical instructor in the UCSD psychiatry department since 2001. She practices psychotherapy and is a clinical supervisor specializing in gerontology, behavioral medicine and student health.
Essential Skills for Disasters: Resilience and Self-Care
by Deborah Hopper, Ph.D.
RESILIENCE
The APA “Resilience” campaigns began after the 9/11 terrorist attacks when it became apparent that the general public was looking for ways in which they could build resilience “in the face of adversity, trauma, tragedy, threats or…significant sources of stress.” (American Psychological Association; https://apa.org). APA partnered with the Discovery Health Channel to create a documentary, as well as a resource tool kit for psychologists to take into their communities and hold resilience-building forums for the public. Resilience is taught by disaster mental health psychologists and clinicians during American Red Cross volunteer trainings. As therapists, we can apply the principles to ourselves, model, and disseminate these skills to our patients. With our country’s ongoing tragic natural and man-made disasters, continued involvement in war, and recent threats of international nuclear war, the need for building our own and others’ resilience remains vital.

Art by obsoleteworld
Resilience, i.e., “bouncing back” from adversity and difficult experiences is a quality present in most people. However, resilience is not a static trait, but rather, a range of “behaviors, thoughts and actions that can be learned and developed.” Resilience helps any individual in their life generally, and is important for any psychologist or behavioral health clinician to cultivate because of the work we do, especially when we treat patients who have experienced trauma. As a result of facing our own life’s challenges and vicariously, those of our patients, over time many of us learn the necessity of strengthening our ability to adapt well. The purpose of this article is to make you aware of the professional resources that you can review in order to build your personal resilience over time. Building resilience may be considered a vital part of our well-being; taking care of ourselves has to be our first priority, as we provide care to others in both our personal and professional lives.
The APA website has a comprehensive document entitled, “The Road to Resilience” that also has a printable format. It covers component areas of resilience, such as factors, strategies, ways to build resilience, learning from your past, staying flexible, and so forth. Although resilience may be built by a combination of factors, research demonstrates that the primary contributing factor is the presence of caring, supportive relationships within and outside the family. Resilience is bolstered by relationships that create love and trust, provide role models, and offer encouragement and reassurance.
The APA has identified ten ways to build resilience, with a sample action step for each:
- Make connections with others – accept help and support from those who care about you.
- Avoid seeing crises as insurmountable problems – change how you interpret and respond to highly stressful events
- Accept that change is part of living – if certain goals are no longer attainable, accept this and focus on circumstances you can alter.
- Move toward your goals – develop realistic goals and ask yourself “What’s one thing I know I can accomplish today that helps me move in the direction I want to go?”
- Take decisive actions – act on difficult situations as much as you can, instead of detaching from problems and wishing they would go away.
- Look for opportunities for self-discovery – seek to learn something about yourself as a result of coping with an adverse situation; many find they’ve grown in some respect.
- Nurture a positive view of yourself – develop confidence in your ability to solve problems and trust your instincts.
- Keep things in perspective – even when facing painful events, try to consider the stressful situation in a broader context and keep a long-term perspective.
- Maintain a hopeful outlook – expect that good things will happen in your life. Try visualizing what you want rather than worrying about what you fear.
- Take care of yourself – pay attention to your own needs and feelings (also see self-care section, below)
Additional ways of strengthening resilience include journaling, meditation, and spiritual practices as ways some people build connections and restore hope.
SELF-CARE
You will notice that “taking care of yourself” is number 10 on the list of ways to build resilience. For behavioral health providers, there are specific tools and strategies to consider implementing, as our field uniquely impacts each one of us. For those of you who are members of the APA Practice Organization, see “An Action Plan for Self-Care,” and additional research-based, in-depth articles on self-care.
In 2016, APA published an article on “Seeking More Balance”, which offers these strategies:
- Practice mindfulness: “…Develop a reflective habit of checking in with ourselves at least a couple times a day, taking note of the emotional ‘weather’ without judgment.”
- Look for silver linings: when working adults–especially women–looked for benefit in negative situations, “they experienced fewer negative psychological effects from work-family conflict.”
- Draw from positive psychology: “Positive emotions…broaden cognitive, attentional and behavioral repertoires…which boosts resilience and facilitates well-being.”
- Take advantage of social support: seeking support from others is critical to well-being
- Seek out good supervisors: sympathetic bosses can be helpful by buffering stress
- Get moving: exercise boosts mood in the short term, and “can improve symptoms of depression, anxiety, addictive disorders and cognitive decline” in the long term.
- Go outside: time spent in nature is linked to improved cognition, attention, mood and subjective well-being, as well as reducing symptoms of stress and depression
- Make your life meaningful: “We do our best work and live our best lives when we have a sense of meaning – a feeling that what we do extends beyond us and brings good to others.”
Of course, no information about resilience or self-care is useful unless we apply it. Perhaps in your professional resilience journey you have learned the necessity of self-care and are doing a good job of it, but if you haven’t started addressing some of the important components mentioned above, please consider a way to encourage yourself to make enhancing both resilience and self-care a continuing priority over time.
I sincerely hope this article has underscored the need for building your own resilience and has inspired you to try and new strategy to enhance your continuing efforts to build resilience and practice self-care.
Links to documents referenced in the article:
- An introduction to the APA’s Resilience campaign: http://www.apa.org/practice/programs/campaign/resilience.aspx
- The Road to Resilience (APA): http://www.apa.org/helpcenter/road-resilience.aspx; en Español: http://www.apa.org/centrodeapoyo/resiliencia-camino.aspx
- Tips for Self-Care (APA Practice Central): http://www.apapracticecentral.org/ce/self-care/acca-promoting.aspx
Print a copy of this article here.

Dr. Hopper specializes in working with the Red Cross as a Disaster Mental Health Volunteer. She is also a Voluntary Clinical Instructor at a UCSD Student-run Free Medical Clinic, and has a part-time private practice working with Veterans and older adults.
President’s Corner
by Annette Conway, Psy.D.
On October 2nd, 2017, Americans woke up to the horror of one of the worst mass shootings in U.S. history. This was, and continues to be a stark reminder of how often we have witnessed similar tragedies unfold in recent times. Among the many who experience vicarious trauma from such events are helping professionals, including (but not limited to) paramedics, police officers, physicians, nurses, lawyers, social workers, and psychologists who work with the victims and their loved ones. We often focus on our professional responsibilities by listening to our clients recall traumatic experiences, which in turn may affect our thoughts, feelings, and behaviors. Working with trauma survivors can shift our beliefs about the world as a meaningful and safe place. One way we can reduce the risk of vicarious traumatization is to ensure we are taking time for self-care. Avoiding isolation and connecting with professionals who understand the experience of working with trauma is helpful, as in maintain a healthy lifestyle consisting of exercise, healthy eating, meditation, yoga, spending time with loved ones, listening to music, taking time off from one’s practice, and, so forth.
Image credit: https://pro.psychcentral.com/child-therapist/2014/09/self-care-for-therapists/
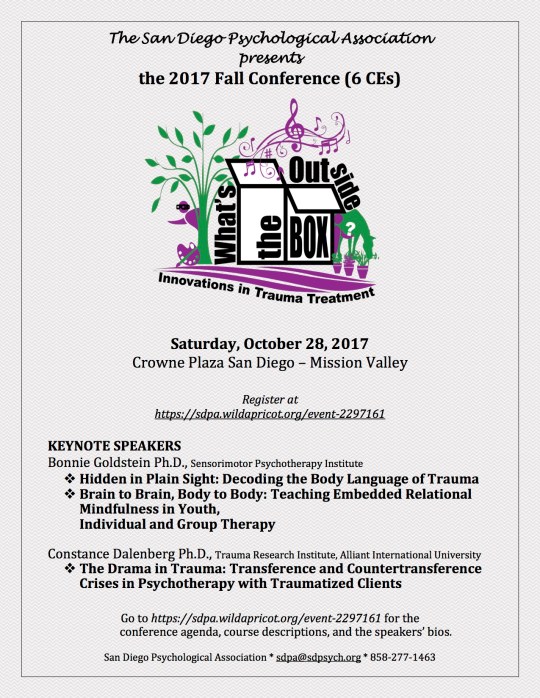
The 2017 SDPA Fall Conference entitled, Innovations in Trauma Treatment: What’s Outside the Box? is another helpful resource in understanding trauma, helping those affected by trauma, and preventing trauma contagion. We have 19 distinguished speakers and 20 exhibitors, along with activities such as yoga, massage, live music, a book raffle table, exhibitor Bingo, and a casual networking buffet lunch. Dr. Bonnie Goldstein, a senior trainer of the Sensorimotor Psychotherapy Institute, and Dr. Constance Dalenberg, Distinguished Professor of Psychology at Alliant University, will be the Keynote Speakers. We welcome you and look forward to offering you a stimulating agenda of continuing education, professional development and networking opportunities.
The Holiday Party/SDPA Awards Ceremony/Installation of the 2018 Board of Directors will be held on Sunday, December 10, 2017. The event is Free to all members and one guest, with the purpose of enhancing our professional and social networks. Giving the awards is a way SDPA can recognize and encourage excellence in the mental health field, as well as build better relationships with the community at large. The Awards that will be presented are as follows:
- Distinguished Contribution to Psychology
- Volunteer of the Year
- Media Award
- Legislative Award
- Fellows Award
We would love to see you there.
In continuing with the theme of trauma and its treatment, our last issue of the year will address some of the pressing issues in our country right now. We would like to feature articles that talk about the role of mental health professionals in disaster relief efforts and helping fellow Americans cope with these uncertain political times. Thank you to those who have already contributed. We hope to hear from more of you, soon.
Dr. Conway is a clinical psychologist in private practice and the President of the San Diego Psychological Association.
Editorial
“I became what I am today at the age of twelve, on a frigid overcast day in the winter of 1975. I remember the precise moment, crouching behind a crumbling mud wall, peeking into the alley near the frozen creek. That was a long time ago, but it’s wrong what they say about the past, I’ve learned, about how you can bury it. Because the past claws its way out. Looking back now, I realize I have been peeking into that deserted alley for the last twenty-six years.” (Khaled Hosseini, The Kite Runner)
There have been times in our recent history that have been marked by a collective sense of great uncertainty, tumult, fear, and despair; this moment in history is no different. Whether it is the fallout from discriminatory public policies, prejudice toward minority and refugee populations, or the barrage of natural disasters in close succession, the lives of an overwhelming number of people are at stake. At the time of this writing, more than 65 million people (source: NPR) are displaced from their homes in Syria, Afghanistan, Lake Chad, Sudan, Myanmar, not to mention those closer to home–from Hurricanes Harvey, Irma, and Maria, the earthquake in Mexico, or the California wildfires.
As these global tragedies continue to unfold, millions of children and adults are facing personal horrors every day, sometimes in their own homes. As psychologists, most of us, at some point in our careers, have been sought out by individuals who are hoping to make sense of their traumatic experiences, whether due to childhood abuse or neglect, sexual assault, violence, automobile accidents, or death of a loved one. Regardless of whether the trauma was chronic or acute, it has the power to shape lives, often unconsciously, and underlies emotions, actions, life choices, and relationships. As we know, trauma is multifaceted, as is the response to it.

Image credit: http://www.lassiterfineart.com/m-tingol/cbexcp9n3jfjggkt8h18kg2as0tsqu
This issue of The San Diego Psychologist is published in conjunction with the 2017 Fall Conference of The San Diego Psychological Association entitled, “Innovations in “Trauma Treatment: What’s Outside the Box?”. I am grateful to Mary Mulvihill, Ph.D., the SDPA CE Chair, who personally reached out to some of our authors to encourage them to contribute to this issue.
The seven articles featured here are diverse, covering a range of topics: Dr. Goldstein (one of the keynote speakers at the Conference) has written about the use of play in group therapy with adolescents; Dr. Collins (SDPA board member) has eloquently described the role of trauma in couples therapy. Dr. Sterling has described her innovative mindfulness yoga course for patients with trauma; Dr. Trim has written a highly informative article on the treatment of trauma among eating disorder patients, a population that is currently underserved; Dr. Shibley’s poignant essay on her own experience as a Dreamer highlights the trauma of having to navigate a hostile and broken immigration system; Dr. Kao has transcribed her interesting interview with Dr. Sidney Zisook, a psychiatrist at UCSD who studies Complicated Grief and its treatment. Finally, we have the honor of featuring Dr. Stevens’ poem about coming together in the face of tragedy—his first-hand account of conducting therapy with the victims of Hurricane Irma will be published in the next issue of the Newsletter, coming out next month.
You may have noticed that we skipped the Summer issue of the Newsletter; we continue to struggle with poor response rates to our call for articles, and have sought to remedy that by reaching out directly to individuals in the SDPA community for articles. (We may be coming for you next!) Voluntary submissions, as always, will gladly be considered for publication. The last issue of the year will come out at the end of November, and continues in the theme of trauma with regard to current events. We are hoping to feature articles about our role as psychologists in disaster relief efforts, as well as in helping patients cope with the current political climate in our country. Please consider writing and making your voice heard!
Please share your feedback in the comments below, or email me with your submissions at TheSanDiegoPsychologist@gmail.com.
Thank you for reading.
–Gauri
 Dr. Savla’s private practice in Encinitas, CA is focused on seniors with aging-related challenges and/or mental illness. Before devoting her professional life to clinical service, she studied primary psychotic disorders among older adults at the University of California, San Diego and the VA San Diego Healthcare System. She has co-authored 30 peer-reviewed papers and book chapters to date. She has been the Editor of the San Diego Psychologist since 2016.
Dr. Savla’s private practice in Encinitas, CA is focused on seniors with aging-related challenges and/or mental illness. Before devoting her professional life to clinical service, she studied primary psychotic disorders among older adults at the University of California, San Diego and the VA San Diego Healthcare System. She has co-authored 30 peer-reviewed papers and book chapters to date. She has been the Editor of the San Diego Psychologist since 2016.
Mindfulness and Play in Group Therapy for Conflict-Resolution among Adolescents
by Bonnie Goldstein, Ph.D.
This article is a modified excerpt from the chapter, “Cultivating Curiosity, Confidence, and Self-Awareness through Mindful Group Therapy for Children and Adolescents,” in Play and Creativity in Psychotherapy edited by Marks-Tarlow, Solomon, and Siegel (2017).
Group therapy harnesses the desire to connect, belong, and feel part of a community, as members’ reflections about their interactions lead to insight and growth. This is especially true in young people who may not have had many opportunities to feel accepted and validated by others, which can reinforce mistaken beliefs about self and others. Young people who avoid others to avoid trauma, wind up isolating themselves from the even the relationships they need to heal and grow. Transformative moments begin with misreading another group member in the here and now, which may evoke feelings from past experiences and relationships. Capitalizing on such interchanges can lay the foundation for repair and resilience, social-emotional development and growth, and the cultivation of curiosity, creativity, and confidence.
Innovative and integrative group therapy comes about through co-creating a playful, safe, nurturing, growth-oriented therapeutic environment in which it becomes less shameful to show hidden parts of the self. Participants in group therapy can reassess their sense of self in relation to others, and gain reassurance as commonalities between members become evident, thus laying the foundation for shifts in experience. Observing changes in other group members can be helpful for those who cannot put into words their own thoughts, feelings and fears. Healing occurs as recognition, exploration, and resolution of trauma and developmental issues during the group experience are aided by an essential element of play, i.e., inviting curiosity. Mindfulness through playful queries such as “I’m curious” or “I wonder” offers a collaborative lens that welcomes wondrous and engaged curiosity, foundations in mindfulness practices, and fosters a deepening awareness of the present moment experience.

The Argument (art by Fredrick Hendrik Keammerer)
Creative and playful interventions to elicit mindfulness help to navigate complicated and contentious relationships, such as will be described in the case example of Danielle and Ian, two teen group members.
Danielle
As a young child, Danielle emigrated from the Middle East with her mother after a change in government regime resulted in their lives being threatened. That was the last time she saw her father, who remained behind. Danielle experienced even greater trauma following September 11, 2001, when both her first and last names were changed. In the ensuing months, her family and others in their community experienced an upsurge of hostility, rage, and racial profiling. These experiences led Danielle to become fearful of others and hesitant to engage with her peers, resulting in her feeling marginalized and rejected.
Danielle was referred to me for her depression by her school counselor, and we began intensive one-on-one therapy as she was beginning 12th grade. I suggested that group therapy could help her combat her sense of isolation as well as aid in developing awareness of the overarching impact of her traumatic experiences. Danielle was wary, but she agreed to give it a try.
After initial resistance that required “curbside therapy,” i.e., meeting Danielle where she needed to be, we decided that she would enter the group with me, so she would not have to make conversation or face her peers alone. Danielle’s body stance implicitly let all members know of her hesitancy; she entered the room with her head down, arms crossed, appearing defiant or avoidant. Her initial responses to group members were curt, often one-word answers to their questions. There was no eye contact. At the time, Danielle seemed unaware of her self-protective stance, which she later recognized as “body armor.”
In a future meeting, group members were invited to share their experiences of one another. Addressing questions ranging from “What was your first impression of group?” to “What was your first impression of one another?” members developed insight and perspective, which led to more sensitivity toward each another. Danielle received feedback suggesting she shift her “body armor” so as to appear less alienating. A large, full-length mirror was brought out so Danielle could view herself in the stance we were discussing. Others also gazed in the mirror, supported by their peers, encouraged by the leaders, in what became a fun and interactive exercise providing much insight.
Danielle’s “body armor” had led to her isolation from her peers, which was exacerbated by her avoiding school clubs and teams, eating lunch alone in the library, and dodging opportunities to be with other students, lest they initiate conversation. In a social-feedback loop, her sense of isolation was maintained by her lack of insight into her avoidant behavior and the lack of tools to break out of this cycle.
As the group progressed, Danielle started to feel safer, both with people and with her own experiences, which slowly led to a sense of stability and confidence around others. She attained a better understanding of her body language and her own thoughts and feelings. This dyadic resonance went beyond simple mirroring to serve as the first step of a feedback loop that facilitated self-understanding. Danielle joined her peers in co-creating a safe environment by talking and listening, and supporting each other. Her intersubjective experience shifted, illustrating how the “group psychotherapy format offers an experiential immersion that fosters awareness and exploration of the ways we know and have a sense of the known within our subjective experience of being alive” (Goldstein & Siegel, in press, p. 260).
One group exercise focused on bringing members’ attention to their body-based experiences (e.g., noticing feelings of curiosity about a new member) or becoming aware of aches in their stomach, legs, and feet (perhaps an urge to mobilize or run). For Danielle, the impulse to bolt could be identified with a tingling in her feet. She noticed her limbs would begin to move and wiggle, which she connected to her instinct to flee the room.

Art by Peter Hansen
As our group sessions progressed, the members became keener interpreters of their inner body and mind signals, for a large part due to the relational component of the collaborative work. Over time, Danielle was encouraged to lead other members in brief breath-work exercises. Taking a turn leading the group in breath-work further deepened her self-confidence and inspired a growing curiosity about other’s experiences.
Learning to be more centered and finding equanimity through these self-calming exercises, which were introduced in a playful manner, Danielle and her fellow group members developed tools to mitigate feelings of shame, anxiety, fear, etc. Leading these exercises helped Danielle deepen her subjective experience and enhance her own integrative capacity, which prepared her for her conflict-ridden interactions with Ian.
Ian
Ian’s ongoing interpersonal challenges and outbursts led his family to bring him to therapy so he could develop self-reflective skills and self-regulation strategies. In the months leading up to the 2016 presidential election, the issues of intolerance, separateness, inclusion, and belonging that were arising nationwide also arose within the therapeutic milieu. Ian, seemingly influenced by the political rhetoric, openly taunted his classmates, especially those whom he perceived as “different.” He proclaimed that he would help “build that wall,” arguing “some people don’t belong here.” Ian seemed to not understand the implications of his behavior, nor was he aware that it may have originated in his own experience of being a target of bullying. (It was later revealed that Ian had been teased and called a “mutt” by peers because of his olive skin and mixed ancestry.)
Ian’s attention-seeking behavior ranged from occasionally positive (bringing pumpkin cupcakes for his group mates) to frequently negative (using derogatory language, e.g., “dumb blonde” in reference to group members, or expressing oppositional or offensive opinions).
One of Ian’s targets of aggressive behavior (shoving, pushing) and verbal taunts was Danielle. After the 2016 election results, he championed the president-elect and called his co-members with opposing political views, “dumb” and “idiots.” He would yell “Make America Great Again” and “Build the Wall” in Danielle’s direction to purposefully trigger her insecurities about her otherness.
To address the escalation of conflict in the group, I directed their attention to explore the meaning Ian ascribed to his comments. I also aimed to illustrate to Ian that he was recreating the type of interpersonal conflict that occurred frequently at his school. This required looking at the moment-to-moment experience transpiring within the group milieu.
One strategy of de-escalating conflict is the “Power Pause.” The group knew that it was time to “down-regulate” when I stood up and indicated a stop sign with my hand, while whispering “Power Pause.” This encouraged group members to examine their own thoughts and feelings and how they were experienced in their bodies: were they feeling more nervous, anxious, more awakened, or numb as the conflict within group escalated? Some observed with wide-eyed panic (perhaps a flight or freeze response, perhaps reminiscent of other conflicts in interpersonal relationships), while others reacted by matching anger, in ever-escalating verbal assault (fight response). By regulating the pace and flow of the group dialogue, group members felt assured of being safely guided through these interactions with support and reinforcement.
Over time, Ian benefitted considerably from supportive positive feedback; his appearance shifted from the confident/cocky bully-rebel, off-putting teen to a more vulnerable, accessible person. This change manifested physically. For example, as he shrugged, Ian’s shoulders dropped forward, his eyes turned downcast. At these times he displayed a fleeting, palpable unease and sense of unworthiness. Often he found these feelings intolerable and would create a minor conflict or use his body provocatively, pushing boundaries or instigating interpersonal conflict to shift the moment or cause a distraction. Ian longed to be seen, recognized, honored, and respected, and these softer feelings were manifested over time in the group.
One way in which I led Danielle and Ian to address the conflict between them was through an interactive Sensorimotor Psychotherapy exercise that uses therapy balls. Danielle and Ian were asked to sit on two large therapy balls placed on opposite sides of the room. They could use gentle bouncing or soothing swaying movements, with feet pushing down on the ground. Gentle bouncing releases tension because it keeps one’s feet firmly gripping the floor in order to balance, and the gentle movement can be calming.
Danielle and Ian were asked to select locations where they could gaze at one another, but at a distance they co-created. Once they found their positions, their conversation continued as they sat on the ball. Another brief hostile interchange was interwoven with playful giggling as one fell slightly off the ball and had to reestablish balance. Some wobbliness ensued, as each was encouraged to find a distance between them that felt correct. Danielle moved back until she was outside the room, at which point Ian said, “that’s right…out…no more group for you”. Our office doors are glass sliders, so Danielle’s annoyance was visible as she sat on her ball without commenting on his incendiary words. Only after Danielle had moved far outside the group room did Ian indicate with his hands that she should stop (the glass “barrier” seemed to serve the function of offering safety).
At that juncture both Danielle and Ian were instructed to notice what they felt in their bodies. I asked body-oriented questions to encourage present moment awareness, including “What do you feel inside your body right now as you face one another?”, “What is happening in your stomach now?” or “Do you feel the anger now that you mentioned feeling earlier?” Although Ian started to recognize that perhaps he had sent Danielle too far away, he seemed to have difficulty suggesting she come forward. He was encouraged to notice what happened when he invited her back into the room with only his eyes and his hand gestures. Peering through the glass, his hesitancy was palpable. As they cautiously and slowly continued the exercise, this time coming closer, Ian acquiesced that he had feelings of anxiety when beckoning her near. Danielle, however, came to a different realization. She said that she had become accustomed to lots of personal space through years of aloneness, and she was not so quick to move back into the group room. She noted that she could breathe more easily when there was plenty of space between her and Ian. She expressed that Ian continued to intermittently remind her of others who had taunted her, and said that she preferred to observe group from outside the glass, looking in.
Little headway was made with respect to their interpersonal conflict until we were able to bring their implicit experience of one another into the room, by examining the underlying process and feelings underlying the conflict. The slower pace allowed for curiosity about what was happening in the present moment, and opened space for members to share their thoughts and feelings, emotions and cognitions amidst the contentious and argumentative banter. As the exercise continued, I instructed Ian to ask Danielle to slowly move towards him, while he remained seated on the ball, until he felt that she was just the right distance from him. In the spirit of curiosity, he was encouraged to use his hands as guides, which he did, albeit reluctantly. After a few moments, the exercise shifted their experience of one another, dispelling the tension over Ian’s comments. In time, Ian apologized for his abusive comments toward Danielle.
The support and respect Danielle garnered during her experiences in group therapy led to shifts in her sense of self in the world. This playful group experience encouraged Danielle to reach out to others at school. Her subsequent evident growth in confidence and willingness to risk being “seen” were clear manifestations of growth based on her group experience.
In this exercise, through the lens of curiosity and playfulness, the collaborative group experience offered connecting and redeeming opportunities that emerged as members shared with one another, as guided by the support of the group leaders. While the tension in the room continued, some members spoke out against Ian’s political beliefs; others offered words of support to Danielle (a unique and gratifying experience for her). In this safe atmosphere, both members could take personal risks, revisit their challenging beliefs, and have an authentic learning experience.
Similar playful exercises are often useful during high-conflict moments in group, allowing for mindful self-awareness to develop, in the present moment, with opportunities for practice, reinforcement, and new cognizance. Please refer to the book chapter for details.
Conclusion
Working with adolescents in the group milieu creates new possibilities for interactions, self-understanding, and confident engagement with others. This is especially important in an environment where politics and prejudice have found their way into the lives of young people. Cohesive therapy groups can thrive when members are kept emotionally safe within the group despite the inevitable interpersonal conflict. The group can model acceptance by not ostracizing anyone or by not allowing a member to be exiled or “killed off.” By prioritizing playful communication and movement exercises, group members can explore emerging internal conflicts, become more mindful of their moment-to-moment experience, and delve beneath the verbal content of presenting problems. All of this can lead to qualitative and quantitative healing and growth, as new neural pathways are created. Healing occurs when we understand how prejudices are mirrored in the body and how they prevent us from both feeling accepted and accepting others.
Print a copy of this article here.
 Dr. Goldstein is a Child and Adolescent Consultant for the Lifespan Learning Institute and a faculty member of the Sensorimotor Psychotherapy Institute, both located in Los Angeles, CA. She is an expert on the Sensorimotor Psychotherapy approach of treating children, adolescents, and families. She is the author of several publications, including Understanding, Diagnosing, and Treating Attention Deficit Disorder/Hyperactivity Disorder in Children and Adolescents, The Handbook of Infant, Child, and Adolescent Psychotherapy: A Guide to Diagnosis and Treatment, Volumes I & II, A Text for Children and Their Families, I Will Know What to Do: A Guide to Dealing with Trauma, and so forth.
Dr. Goldstein is a Child and Adolescent Consultant for the Lifespan Learning Institute and a faculty member of the Sensorimotor Psychotherapy Institute, both located in Los Angeles, CA. She is an expert on the Sensorimotor Psychotherapy approach of treating children, adolescents, and families. She is the author of several publications, including Understanding, Diagnosing, and Treating Attention Deficit Disorder/Hyperactivity Disorder in Children and Adolescents, The Handbook of Infant, Child, and Adolescent Psychotherapy: A Guide to Diagnosis and Treatment, Volumes I & II, A Text for Children and Their Families, I Will Know What to Do: A Guide to Dealing with Trauma, and so forth.
Relationship as a Developmental Trauma: Healing Directions in Couples Therapy
by Linda Collins, Ph.D.
History taking with couples often reveals a childhood wherein the chronic relational experiences with one or both parents led to an environment that was emotionally unsafe, unpredictable, and unreliable. This developmental history might suggest an attachment disorder impacting future adult relationships. Is this condition also a form of developmental/relational trauma?
Dr. Bessel van der Kolk, identified a condition in 2005 that has been referred to as Developmental Trauma Disorder (DTD). This condition, not formally recognized in the DSM-5, is defined as living in general anxiety or non-stop terror before the age of three. This kind of trauma occurs prior to the frontal cortex coming on line and cannot be recalled as a discrete event. Van der Kolk identifies the symptoms of DTD as relational and chronic: the inability to concentrate or regulate feelings, chronic anger, fear, and anxiety, self-loathing, aggression, and self-destructive behavior.

Art by John Bull, 1950 (http://www.imagekind.com/art/stunning/arguing/drawing/fine-art-prints)
Van der Kolk (2005) identifies insecure attachment and attachment disorder as the cause of developmental trauma. Diagnosing DTD can only be made on the basis of the symptoms, since the defining experience of trauma occurs before it can be recalled. These symptoms are often somatic and not linked to event memories.
Another diagnosis that has been adopted by the traumatic stress field is Complex Trauma Disorder (Aideuis, 2007). Complex trauma (also not recognized formally in the DSM-5) is used to address “the multi-faceted nature of trauma experienced by children when violence, neglect and fear form the fabric of their early existence” (Aideuis, 2007). Seven domains of symptoms make-up this diagnosis, including insecure attachment issues, sensory processing issues, emotional regulation issues, alterations in states of consciousness, problems with behavioral control, cognitive difficulties, and problems related to self-concept.
The case example below illustrates the clinical presentation of relational experiences after the age of three that are remembered as emotionally unsafe and frightening. Both partners in the couple described below have trauma histories that include difficulties with experiencing emotional safety and the reliability of getting their needs met in their caregiving relationships. One of the partners has a history of other trauma, including early sexual abuse and witnessing the death of two friends, one by suicide.
Michael and Sherry (names changed for confidentiality) have two children, aged 4 and 6 years. Their son, 4, just started in a transitional kindergarten program. He has been diagnosed with ADHD, is very active, and has a hard time following directions and sitting. Sherry describes, with increasing irritation, that she has been trying to set up a meeting with her son’s school to deal with his special needs, and that they have not responded.
Sherry continues focusing on her concerns in this couples therapy session about her son, listing the ways in which the school staff “doesn’t care about his needs” and their lack of response to her emails. Sherry’s voice begins to shift from irritation and anger to reflect her fear and hurt. Tears form in her eyes. Michael, in an attempt to diffuse the increasing emotion, offers an explanation that the school has a lot on their plate and may simply be delayed in getting back to them. Sherry is triggered by Michael’s suggestion and reads his tone as a judgment about her concerns and reacts defensively. Michael begins to feel triggered by Sherry’s defensive response, which he perceives as an attack. His efforts to help, he feels, have been rejected and misunderstood.
Both partners appear to be caught in a relationship interaction that felt reminiscent of chronic relational misattunements and emotionally unsafe relationships during their childhoods. During the intake, Michael revealed that he was sexually abused at 4 years of age by his brother’s friend. His father was described as quick-tempered, as was his mother. Michael began to get severe panic attacks at age 23 and has also been diagnosed with Attention Deficit Disorder. He has also struggled with depression most of his life.
Sherry describes growing up with a mother who was preoccupied with her own work life. Sherry felt perpetually blamed for not doing things the right way. She began using drugs in her adolescence, but has currently been sober for 16 years. She has struggled with depression, and in 2015 was diagnosed with rheumatoid arthritis and fibromyalgia.

The ways that the couple described above get “stuck” can be understood more clearly through the lens of the complex relational trauma that both partners experienced. Susan Johnson (2002) in her book, “Emotionally focused Couple Therapy with Trauma Survivors” points out the importance of beginning to work with couples as described above, by using past events and experiences to “validate the self protective stances partners are taking in the present relationship.” Janina Fisher (2017) approaches the beginning of treatment by explaining the neurobiology of trauma and helping the couple to see their trauma as the villain rather than one another. Framing past trauma as their adversary has proven to be very helpful for Sherry and Michael; they could unite around this understanding rather than personalize the trauma-informed reactions.
Sue Johnson (2002) also suggests that therapy with trauma survivors may include the following stages of intervention. Stage 1 comprises stabilization where safety is established, and the couple understands how the effects of trauma and lack of security shape their responses to one another. Stage 2 is focused on restructuring the bond between partners, and Stage 3 is focused on a process of integration.
The case example above demonstrates how trauma history of one or both partners shapes and contributes to their relational problems. The emerging diagnoses of Developmental Trauma Disorder and Complex Trauma Disorder offer the clinician a way of understanding early trauma that does not fit into the more event-oriented trauma of the Post-traumatic Stress Disorder (PTSD) diagnosis.
Intervention models such as Johnson (2002) and Fisher (2017) reflect the need to alter the couple treatment approach based on an understanding of the trauma histories of one or both partners. Validating the defensive responses of both partners shaped by their trauma histories models compassion and understanding for both partners. Integrating a psycho-educational approach to understanding trauma and the dysregulation of the nervous system in response to trauma can help each partner to depersonalize some of the automatic and reactive responses received from their partners.
References
Aideuis, D, (2007), Promoting Attachment and Emotional Regulation of Children with Complex Trauma Disorder, International Journal of Behavioral Consultation and Therapy, Vol.3, No.4, pp.546-554.
Fisher, J. (2017), Healing the Fragmented Selves of Trauma Survivors, Routledge.
Johnson, S. (2002), Emotionally Focused Couples Therapy with Trauma Survivors, Guilford Family Therapy Series.
Van der Kolk (2014), The Body Keeps the Score-Brain, Mind and Body in the Healing of Trauma, Penguin Group.
Van der Kolk (2005), Complex Developmental Trauma-Editorial Comments, Journal of Traumatic Stress, Vol.18, Issue 5, pp.385-388.
Print a copy of this article here.

Dr. Collins has completed advanced training with the Gottman method of couples therapy. She is certified as a Somatic Experiencing Practitioner and specializes in working with individuals and couples with a trauma history.
Mindfulness Yoga for Trauma: A New Approach to Trauma Treatment
by Dianne Sterling, Psy.D.
The concept of traumatic stress and PTSD is a relatively new one. Initially called “gross stress reaction” in the DSM after the Second World War to describe symptoms in veterans, it expanded to include other forms of trauma and labeled PTSD in the 1980 DSM-III. In the 1980s and 90s, PTSD symptoms were linked with the survival response of the nervous system, supporting the physiological underpinnings of the PTSD response.
Since then, prolonged exposure therapy and cognitive processing therapy (CPT) have been researched and heavily utilized for trauma treatment. Other approaches also emerged, such as EMDR. SSRIs and other antidepressants have been commonly prescribed as well. In the past 20 years, the understanding of trauma has expanded to include complex trauma, which involves chronic interpersonal trauma exposure, particularly during early development. Judy Herman, M.D. and Bessel van der Kolk, M.D. have been pioneers in expanding the understanding of traumatic stress to include trauma caused interpersonally.
Functional Magnetic Resonance Imaging (fMRI) research has greatly contributed to the understanding of the neurobiology of trauma, and the particular neurophysiological responses including the fight/flight/freeze reaction, sympathetic nervous system and neuroendocrine activation. fMRI studies of the phenomenon of triggering show that most activation occurs in the older and primitive structures of the mammalian and reptile brain.
Recent developments in trauma treatment include strategies that expand beyond verbally based psychotherapy to approaches that integrate the body into the therapy. Enhanced mind/body approaches to trauma treatment such as Sensorimotor psychotherapy and Somatic Experiencing address implicit memory that evokes trauma-related hypo or hyper-arousal. Van der Kolk and colleagues have investigated other bodily-based and holistic ways to heal trauma, including meditation, yoga, and neurofeedback, among others. This research demonstrates that trauma resides in the body and underscores the need for comprehensive treatment that includes the physiological symptoms of trauma. In his recent book “The Body Keeps the Score,” van der Kolk explains how symptoms of trauma are adaptive and survival-based, and tend to get wired in the nervous system and “encoded in the viscera.” Traumatic residue in the body may result in symptoms that are often physical in nature, such as triggering, startling, chronic nervous system over-arousal, and anxiety. Research suggests that the threat system in the brain becomes altered with intense or repeated trauma, including a persistent reactive autonomic nervous system and sensitized endocrine system. Trauma survivors also frequently employ numbing and dissociation, leaving them feeling unsafe and disconnected from their bodies.
“The body keeps the score. If the memory of trauma is encoded in the viscera, in heartbreaking and gut-wrenching emotions, in autoimmune disorders and skeletal/neuromuscular problems, and if mind/brain/viscera communication is the royal road to emotion regulation, this demands a radical shift in our therapeutic assumptions.” (van der Kolk, The Body Keeps the Score, p. 86)
In psychotherapy practice, we frequently encounter patients with trauma. As psychologists, we have many tools to address emotional pain and traumatic memory, but often do not target the somatic symptoms of trauma directly where they live in the body. As someone who has studied and treated trauma for 30 years and followed the work of Drs. van der Kolk, Herman, and others, I have been intrigued the mind/body approach to treatment. However, despite having been a long-term meditator, mindfulness teacher, and yoga practitioner, I found it challenging to implement these approaches in my traditional psychotherapy practice. I have utilized mindfulness tools and tracking the sensations in the body as a source of information to differentiate thoughts, feelings, and body experiences, as well as explaining ways to invoke the relaxation response. Yet, I remained convinced that there was a wider range of somatic interventions that could further help my trauma patients.
Over the years, I have referred patients to MBSR classes (Mindfulness Based Stress Reduction), local meditation classes, and yoga classes. Unfortunately, my trauma patients did not always benefit from them; some reported that breath meditation created anxiety with the focus on the bodily experience of breathing. Others found that certain yoga poses as well as certain actions of the yoga teachers created discomfort, nervous system reactivity, and sometimes brought on an overwhelming sense of vulnerability.
In his work at the Trauma Center in Boston, Dr. van der Kolk had similar experiences when he began researching yoga as a therapeutic modality. In fact, he had a 50% drop out rate in his initial yoga research because of the discomfort it aroused in trauma survivors. This led to the development of Trauma-sensitive yoga with David Emerson, a yoga teacher, so survivors could benefit from the therapeutic aspects of yoga practice without the “side effects” of a traditionally led yoga class. Patients at the Trauma Center were referred to yoga classes on site in addition to their therapy visits.

Yoga (art by Marlene Koenig; available on Etsy)
The principles of Trauma-Sensitive Yoga include not using certain poses that evoke a sense of vulnerability, no adjustments by the teacher, never walking behind students in class, no “commands” or instructions to push endurance, and avoiding certain props. The goal was to create a safe environment that fostered choice and control while allowing survivors to safely connect to their bodies, breathing with movement and quieting the overactive nervous system. David Emerson has documented this refined approach in several publications, and also offers online and in-person training.
Armed with my knowledge of the mind/body research on trauma and available somatic interventions, I developed a carefully choreographed six-week course (currently named Mindfulness Yoga for Trauma) that could be adjunctive to psychotherapy. This course combines didactic information about the science behind the neurobiology of trauma and related topics, with teaching mindfulness and somatic practices, such as Trauma-Sensitive Yoga.
Science and research can drive acceptance and understanding, creating more motivation to use and try mindfulness and yoga practices. Learning and understanding the mechanisms of trauma and what can be done to alleviate symptoms empowers the participant to take charge of their own healing at their own pace. It also has the possibility to “de-shame,” since gaining understanding that the symptoms of traumatic stress are not cognitive, but survival-oriented and originate in more primitive brain structures in our brain. In other words, you cannot “out-think” it; it is an automatic survival mechanism.
The Mindfulness Yoga for Trauma course emphasizes tools for calming, grounding and self-regulation, and no expectation of self-disclosure. It is made clear that it is not a therapy group, but a safe space to learn with the implicit knowledge that everyone present has a trauma history. This course has been taught three times over the course of the last year.
Each of the six weeks is focused on a different topic, and comprises an hour of presentation and an hour of mindfulness training and trauma-sensitive yoga practice. Some topics are didactic only, such as the neurobiology of trauma, polyvagal theory, and how trauma resides in the body. Other topics covered are commonly employed strategies in trauma treatment, such as how to use grounding both cognitively and physically to anchor and establish safety, physical and emotional self-regulation, self-compassion, and post-traumatic growth and resilience. Each topic is followed by a mindfulness exercise or training. The exercises are geared toward observation of sensations without judgment and tracking sensation and emotion to interrupt automatic reactions. This cultivates self-awareness and makes space for self-observation, noticing and befriending what is experienced to reduce the stress response. For those who have disconnected or dissociated, it allows safe reconnection. For those who are physically reactive with triggering and hyper-arousal, it promotes pausing and noticing what is being experienced and eventually interrupting the stress response. Directing attention to the present moment has been proven to increase ability to gain perspective and regulate responses. Resources such as books and webcasts are provided in the handouts. The second hour of each class is a guided yoga session of slow, gentle poses and breathing using the principles of trauma-sensitive yoga. Participants are encouraged to practice mindful awareness while practicing yoga, and to go at a pace that is right for them. They are also encouraged to use grounding if anything becomes triggering and uncomfortable.
At the end of the course, participants are are asked to complete a confidential feedback form. The following are some abbreviated comments that we have received over the last year:
- “I liked the lectures, it made understandable why the yoga and movement helped”
- “When I feel triggered I have been able to use the tools to overcome it, thank you!”
- “Grounding helped a lot”
- “I appreciated not being asked to share or talk about personal trauma”
- “I wanted to let you know that I made the connection of my response to a homeless person. In my sadness, I was able to pause and connect to a former experience in my life when I had to stay in a safe shelter for a month. I allowed my feelings to arise with self compassion, took a breath, grounded, and was able to feel peace and not shame. I’ve learned a lot”
- “I appreciated not being asked to share or talk about personal trauma” “Someday a body-centered mindfulness treatment will be prescribed for most people who suffer serious trauma, like physical therapy after an injury. We will look back and wonder how it was possible to recover without addressing the pain that resides beyond the mind’s reach”
The overall goal of Mindfulness for Trauma is to equip participants with tools and information, heightening perceptivity in the mind/body connection and how trauma impacts functioning. Participants learn to comfortably practice mindfulness and yoga exercises on their own without being triggered or having to look for appropriate yoga classes or courses like MBSR, or MSC (Mindful Self Compassion). This increases understanding, self-awareness and increased capacity to pause, observe and reduce reactivity as well as promotes self-compassion, becoming more present without fear and, of course, reducing symptoms.
Print a copy of this article here.

Dr. Sterling has been in private practice for over 27 years, and a mindfulness consultant for Scripps Center for Executive Health for the last decade. She also volunteers to treat military vets as part of the Give An Hour program and is a long term meditator and yoga practitioner.
